 |
Q:
I’ve recently seen some discussion on treating fungal keratitis with rose bengal and photodynamic therapy (PDT). How does this combination’s efficacy compare with riboflavin and corneal crosslinking (CXL)? Are there any indications for one procedure over the other?
A:
Yes, more than it may seem. “Various methods are available for managing KCN depending on the stage and progression status,” according to Katelyn Lucas, OD, of Price Vision Group in Indianapolis.
Dr. Lucas says early stages can be managed with glasses or contact lenses, while Bowman’s layer transplantation (BLT), deep anterior lamellar keratoplasty (DALK) and penetrating keratoplasty (PK) are performed in advanced cases. She notes that CXL prevents disease progression, and intrastromal corneal ring segments (ICRS) and conductive keratoplasty (CK) reshape the cornea to reduce refractive error.
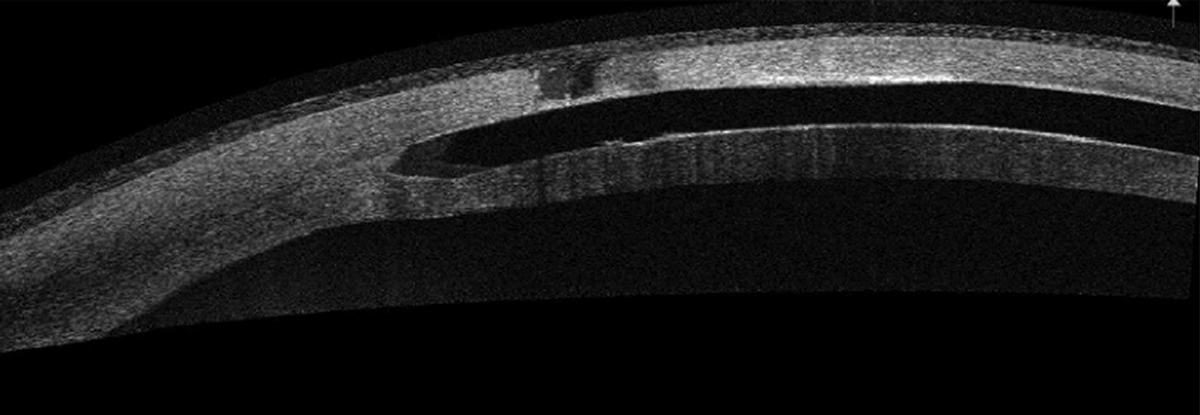 |
| Anterior segment OCT of corneal melt over an ICRS. Click image to enlarge. |
Weighing Your Options
While no universally accepted treatment guidelines exist for ectasia, Dr. Lucas offers her take on the options:
• CXL. Topical riboflavin and UVA light promote the formation of strong chemical bonds between collagen fibrils to strengthen the cornea, notes Dr. Lucas. Studies investigating the standard Dresden protocol have reported high success rates in halting disease progression and decreasing keratometry readings.1 Epi-on CXL has produced inconsistent findings, while an accelerated version of CXL that reduces UV exposure time by increasing irradiance has shown promising results.1 CXL can also be combined with photorefractive keratectomy, thermal keratoplasty, ICRS or LASIK to improve visual acuity.1
Crosslinking has succeeded because it’s effective and minimally invasive. Other choices may have a narrower range of applicability but can play a role in well-selected patients.
• ICRS. These arc-shaped pieces of polymethyl methacrylate are placed within the stroma to help flatten and reshape the cornea in mild to moderate KCN, Dr. Lucas says. ICRS improve visual outcomes by reducing myopia and astigmatism.2 Combined ICRS/CXL can amplify the flattening effect and reduce corneal cylinder.1
• CK. Radio wave energy heats and shrinks stromal collagen, inducing steepening in flat areas and correcting refractive error.3 Off-label CK use for KCN can reshape the cornea, reduce astigmatism and decrease keratometry readings.3 Dr. Lucas notes CK may need to be combined with other procedures to achieve the desired effect, such as ICRS to correct high cylinder and CXL to prevent disease progression.
• IOLs. Contact lens–intolerant KCN patients who have stable disease may benefit from phakic intraocular lenses (IOLs), suggests Dr. Lucas. IOLs can reduce refractive error, myopia and astigmatism in various KCN stages and can combined with CXL, ICRS and corneal transplantation.1
• BLT. This technique reduces ectasia in advanced KCN.4 Corneal ectasia occurs as Bowman’s layer destabilizes, necessitating a graft in the mid-stroma to prevent progression and stabilize the cornea.1 A preliminary study found decreased K readings, improved visual acuity, reduced higher-order aberrations and stabilized disease progression.1,4
• DALK, PK. With thin corneas, significant anterior scarring or nonfunctional vision with contact lenses, a DALK is typically recommended, according to Dr. Lucas. The visual results are similar to those of PK, but the patient’s own Descemet’s membrane and endothelial cells are retained, eliminating risk of endothelial cell rejection and allowing the graft to last the patient’s lifetime. The wound also heals better and faster than in PK, and less topical steroid is needed.
1. Mohammadpour M, Heidari Z, Hashemi H. Updates on managements for keratoconus. J Curr Ophthalmol. 2018;30(2):110-24. 2. Zadnik K, Money S, Lindsley K. Intrastromal corneal ring segments for treating keratoconus. Cochrane Database Syst Rev. 2019;5(5):CD011150. 3. Kato N, Toda I, Kawakita T, et al. Topography-guided conductive keratoplasty: treatment for advanced keratoconus. Am J Ophthalmol. 2010;150(4):481-9. 4. van Dijk K, Parker J, Tong CM, et al. Midstromal isolated Bowman layer graft for reduction of advanced keratoconus: a technique to postpone penetrating or deep anterior lamellar keratoplasty. JAMA Ophthalmol. 2014;132(4):495-501. |
