 |
Q:
I have a few patients with significant anterior segment staining (corneal and conjunctival) who seem to be good candidates for autologous serum. Can you talk about how to acquire these drops and what concentration works best?
A:
LSCD occurs when there is loss of or damage to LSCs or the microenvironment that promotes their survival, according to Katelyn Lucas, OD, of Price Vision Group in Indianapolis. She notes that LSCs are required for corneal epithelialization to maintain surface integrity and corneal transparency.
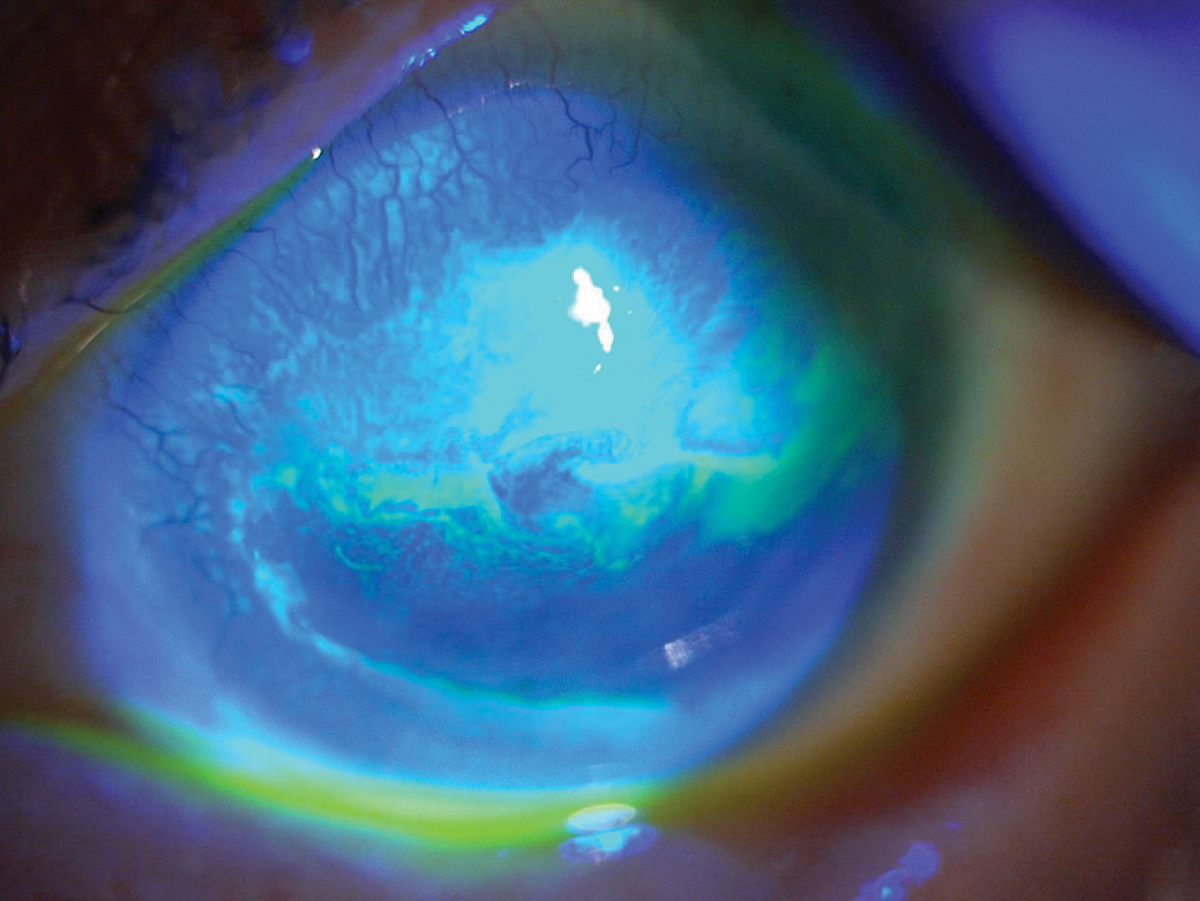 |
| Superior epitheliopathy extends centripetally in a whorl pattern in LSCD secondary to chemical burn. Click image to enlarge. |
The Breakdown
Dr. Lucas notes that partial/sectoral LSCD occurs when a section of the limbus is involved, typically the superior limbus, and can be managed by improving the ocular surface to provide a livable environment for LSCs. Total/diffuse LSCD typically results in surgery, as no LSCs are present to repopulate the corneal epithelium. Primary causes of LSCD result from congenital or genetic disorders, while secondary causes are due to ocular surface disorders or external factors, including CL wear.1
The cause of CL-induced LSCD is likely multifactorial, with potential factors including hypoxia, disinfecting solution, mechanical trauma and dry eye.2 These cases are easily overlooked, says Dr. Lucas, as they are typically mild and patients are usually asymptomatic. It is estimated that up to 5% of CL wearers develop signs of LSCD, with the majority being soft CL users.2 Dr. Lucas recommends conducting a thorough slit lamp exam, as punctate staining may be the only early sign.
Many CL-induced LSCD cases can be reversed with the cessation of CL use, says Dr. Lucas, adding that dry eye therapy can help improve the ocular surface. When conservative therapy is not enough, she suggests considering topical vitamin A, punctal plugs, topical anti-inflammatory meds or autologous serum tears. She warns that severe CL-induced LSCD may require surgical management with autologous or allograft LSC transplantation.
The Process
Autologous serum tears contain a variety of factors that help epithelial cells with proliferation, differentiation and maturation.3 Dr. Lucas notes that concentrations range from 20% to 100%, and dosages can be anywhere from BID to hourly depending on severity. When initially prescribing serum tears, she typically starts with a 20% concentration dosed four to six times daily. If signs and/or symptoms don’t improve or the initial presentation is more severe, she advises prescribing a higher concentration.
Long-term use of concentrations above 50% may slow epithelial growth and increase scarring and inflammation due to serum pro-inflammatory factors.3 Dr. Lucas notes that lower concentrations may be used for years if the patient continues to improve. If LSCD resolves, she recommends discontinuing serum tear use and continuing with conservative therapy to promote a healthy environment for LSCs.
After the patient has blood drawn, Dr. Lucas says they can then take their vials to a compounding pharmacy or a company that partners with local labs. To prevent contamination and degradation, serum tears need to be refrigerated or kept frozen until needed. In diabetes patients, finger-prick autologous blood is a low-cost, accessible alternative.
CL-induced LSCD can be difficult to diagnose due to its subclinical, asymmetric presentation. Clinicians must carefully examine their CL patients, as early intervention can help restore LSC health. When met with challenges in the LSCD management, autologous serum tears are a great tool to treat refractory ocular surface disease.
1. Le Q, Xu J, Deng SX. Review: the diagnosis of limbal stem cell deficiency. Ocul Surf. 2018;16(1):58-69. 2. Rossen J, Amram A, Milani B, et al. Contact lens-induced limbal stem cell deficiency. Ocul Surf. 2016;14(4):419-34. 3. Yeh SI, Chu TW, Cheng HC, et al. The use of autologous serum to reverse severe contact lens-induced limbal stem cell deficiency. Cornea. January 24, 2020. [Epub ahead of print]. |
