 |
In the past 55 years, more than a million corneal transplants have restored vision for patients, and more than 40,000 patients undergo this procedure every year.1 Naturally, these patients will turn to their optometrist for primary care concerns. Caring for these patients is well within the OD’s scope, but they do have special needs, whether those are fitting a specialty contact lens, an annual exam to evaluate the health and integrity of the graft, or a postoperative visit to monitor the healing process. Additionally, these patients may present urgently with decreased vision, redness or other symptoms. Understanding the hurdles and timing that were overcome while procuring the graft should make any process that threatens the graft urgent and paramount to the examining doctor.
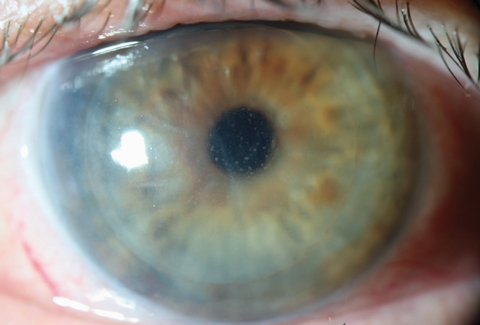 |
| This patient’s DSAEK rejection demonstrates microcystic edema and Descemet’s folds with keratic precipitates. Click image to enlarge. |
Success and Failure
The cornea is an “immune privileged” tissue that is avascular and possesses immune characteristics that allow any suitable cornea to be transplanted from the donor to the recipient, whether ABO or human leukocyte antigen matched.2 Penetrating keratoplasty was the standard for transplantation for dystrophies, infections, scarring and keratoconus, but with the advent of Descemet’s stripping endothelial keratoplasty (DSEK/DSAEK) and Descemet’s membrane endothelial keratoplasty (DMEK), endothelial dystrophies can be treated with less risk for failure and shorter recovery time.3 Although they require greater surgical time, anterior corneal transplants, such as deep anterior lamellar keratoplasty have also significantly diminished rejection rates and enhanced the success rate of corneal transplants.4
Clarifying the terms “rejection” and “failure” is the first step to identifying what process is taking place. Graft failure is a term that describes any reason the graft has stopped functioning and has become cloudy, preventing usable vision. This may be due to any number of reasons, such as endothelial pump failure, rejection, infection or ocular surface disease.5,6 Graft rejection is a specific process whereby the host immune response is directed toward antigens on the corneal donor button.7 Rejection leads to failure, but failure is not necessarily caused by rejection.
Graft rejection is characterized by one or more of these patient symptoms: redness, pain, photophobia and decreased vision. Common clinical findings that could indicate early rejection are corneal edema, corneal infiltrate, anterior chamber reaction, keratic precipitates (specifically on the graft endothelium and not the host) and limbal injection.8 A rejection line is one clinical finding that is pathognomonic for graft rejection. These can be epithelial or endothelial (Khodadoust line).
Rejection Types
Differentiating these clinical signs can help distinguish what type of rejection is taking place. Epithelial rejection occurs at the peripheral edge of the graft and is associated with localized engorged vessels and an elevated epithelial line, or ridge, which stains with fluorescein.8,9 Subepithelial infiltrates, which are whitish and appear similar to those found in viral conjunctivitis, indicate another form of rejection known as subepithelial or chronic stromal rejection.9 This presentation may be confused with viral conjunctivitis and should be considered rejection by the practitioner until proven otherwise to prevent misdiagnosis and further graft morbidity.
The most common form of rejection in up to 50% of cases is endothelial rejection, which is associated with limbal engorgement, corneal graft edema, anterior chamber reaction, keratic precipitates, and a Khodadoust line.10 A Khodadoust line consists of segmented corneal edema and endothelial white blood cells adjacent to an area of clear cornea on the graft, which forms a distinct line.8,9
Understanding the severity of the rejection episode is critical to the survival of the graft. Research shows that following a rejection episode, graft failure is likely to occur in up to one third of these cases within six months.10 One way of categorizing endothelial rejection by clinical findings is into three categories: possible, probable and definite (Table 1).9 A vascularized cornea, especially deeper stromal vessels, is known as a high-risk cornea in transplant patients.9 This is the single greatest risk factor for long-term failure. If a rejection episode is identified, then a phone consultation with the surgeon is always warranted, and these findings will help initiate the appropriate course of treatment and follow up.
Table 1. Endothelial Rejection Severity |
| Possible: Graft edema only. |
| Probable: Edema, cells/flare, keratic precipitates on donor button. |
| Definite: Edema, cells/flare, keratic precipitates on donor button, and Khodadoust Line. |
Options
Treatment of graft rejection depends on the level of comfort of the practitioner, but in all suspected cases, treatment should be administered in consultation with a corneal surgeon. Initial dosage with topical steroids in a known rejection is Q2H with difluprednate 0.05% or Q1H with prednisolone 1%.7,9 This may be given in conjunction with a sub-Tenon’s injection of triamcinolone acetonide and/or oral prednisone initially (40-80mg PO), or possibly an IV methylprednisolone dose of 500mg.7,9 The rate of reversal in severe endothelial rejection is as high as 60% when appropriate therapy is initiated.11 This initial therapy is essential in high-risk patients, and may vary depending on the clinical findings.
Realizing that inflammation is the root cause of rejection, by identifying factors that can contribute to inflammation and further trigger an immune rejection, the clinician can provide the highest level of care to a transplant patient. For example, loose sutures can stimulate inflammation and incite infection and should be identified and removed. Poorly fit post-surgical contact lenses can cause superficial epithelial damage or long-term endothelial damage and trigger inflammation.12 Additionally, conditions such as previous herpetic infection, dry eye, allergies and lid disease/lagophthalmos are just a few ocular comorbidities that can trigger inflammation on the ocular surface.12
All patients who have undergone corneal transplant surgery, regardless of type, should be placed on a daily topical immunosuppressant for life, such as loteprednol or fluorometholone. In cases when the patient is a steroid responder, anti-glaucoma medications can be considered or, in severe cases, a topical cyclosporine may be considered for long-term therapy.
Educating our transplant patients that the earliest detection of symptoms such as pain, photophobia, redness or decreased vision is reason for an urgent visit will also help prevent loss of graft due to poor follow up. n
Dr. Kuc specializes in glaucoma, cataract and dry eye care at Virginia Eye Consultants in Smithfield, VA.
1. Frequently asked questions. Eye Bank Association of America. http://restoresight.org/wp-content/uploads/2015/07/Frequently-Asked-Questions.pdf |
