 |
Q:
I have a 60-year-old patient who gets herpes simplex almost twice a year. Since taking prophylactic Valtrex (valacyclovir, GlaxoSmithKline), she has not had any new outbreaks. She now wants to get Shingrix (glycoprotein E, GlaxoSmithKline). What is recommended here?
A:
Shingrix, a shingles vaccine, was FDA-approved in 2017 for immunocompetent individuals who are at least 50 years old. It is a recombinant, adjuvant subunit vaccine that does not contain live virus. “Because it does not contain live virus, it will likely not be significantly affected by antiviral therapy,” according to Stephanie Klemencic, OD, of Cincinnati Vision Partners and the Cincinnati Eye Institute. “This allows our patients to continue their antiviral medications, such as Valtrex, while receiving this two-dose vaccine.”
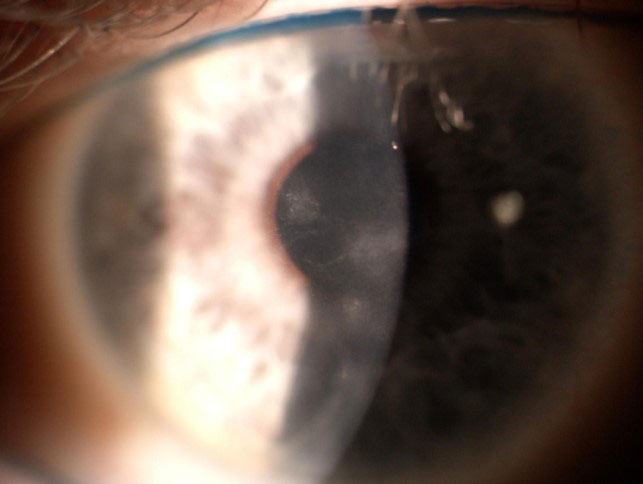 |
Persistent opacities from past herpes simplex events are present in this eye. Click image to enlarge. |
First-line Treatment
On the other hand, Zostavax (live-attenuated vaccine, Merck), the first shingles vaccine, contains live virus. Patients must cease antiviral medication use at least one to two days prior to vaccination with Zostavax and not resume use until at least two weeks later.
As of July 1, 2020, Zostavax is no longer sold in the United States. Some pharmacies and clinics may still have the vaccine in stock and use it until the supply expires on November 18, 2020.
Shingrix is at the forefront of shingles vaccination, as it is almost two times more effective than Zostavax, at around 97%.1 This is one of the main reasons the Advisory Committee on Immunization Practices recommends Shingrix as the preferred vaccine for reducing the incidence of herpes zoster.1
Vaccination with Shingrix should be every clinician’s first line of defense against herpes zoster ophthalmicus, Dr. Klemencic suggests. She recommends encouraging vaccination for patients who are potential candidates to prevent shingles and its complications, including post-herpetic neuralgia, even if they already received the Zostavax vaccine.
Both herpes simplex and herpes zoster can be visually devastating ocular diseases, says Dr. Klemencic. Fortunately, patients have effective options that they can pair with a vaccine, she notes, one of them being antiviral therapy. Long-term suppressive doses of antiviral therapy can reduce the recurrence of herpes simplex virus by 50%, especially in those with recurrent episodes of stromal keratitis.2
1. Dooling KL, Guo A, Patel M, et al. Recommendations of the Advisory Committee on Immunization Practices for use of herpes zoster vaccines. Morb Mortal Wkly Rep. 2018;67(3):103-8. 2. Wilhelmus KR, Beck RW, Moke PS, et al. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. N Engl J Med. 1998;339:300-6. |
