 |
Q: Are severe eye pain and elevated intraocular pressure (IOP) common side effects of a Visian implantable collamer lens (ICL) procedure?
A: The Visian ICL (Staar Surgical) is a flexible phakic IOL made from a biocompatible collagen copolymer that is placed in the ciliary sulcus behind the iris and in front of the natural lens. FDA-approved to correct myopia ranging from -3D to -20D in non-presbyopic adults, the collamer lens is a refractive option for patients looking for an alternative to LASIK or PRK. On average, the out-of-pocket cost is $3,500 per eye.
“One of the most important considerations in ICL selection is the size of the lens relative to the sulcus diameter,” says Linh Hong, OD, an optometric resident at SouthEast Eye Specialists in Chattanooga, Tenn. “A lens that is too long will increase anterior vaulting. Too much vault will crowd the angle, and too little vault can result in anterior subcapsular opacification. Because of the proximity of the optics to the pupil, peripheral iridotomies (PI) are made a week prior to ICL implantation to prevent pupillary block.” Ideally, the ICL vault will be between 250µm and 750µm, or approximately 100% of the corneal thickness.1
Pupillary block and acute angle closure are two uncommon but possible side effects of ICL implantation, says Dr. Hong. Peripheral iridotomy obstruction can occur with healing, blood clot formation or the presence of an undersized ICL. For this reason, experts recommend performing two PIs, in case one becomes occluded or non-functional.2 Acute angle closure can be caused by an oversized ICL, which results in excessive anterior vaulting.2 Excessive vault pushes the iris forward, which leads to appositional closure of the angle, Dr. Hong says. If the PIs are patent, this is likely the cause.
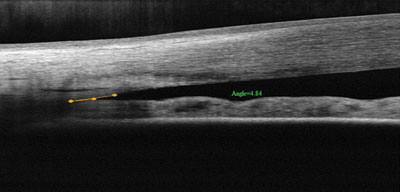 | |
| Pupil block and narrow angle shown in a patient’s left eye on OCT. |
Dr. Hong describes a recent case: a 24-year-old Caucasian female patient presented complaining of severe eye pain, with a history of a Visian ICL implanted nine days prior. The patient’s IOP at the time of the visit was 46mm Hg. Both eyes were implanted, with IOLs displaying excessive anterior vaulting (300% OD, 500% OS). The patient had patent PIs at 11:00 in the right eye and at 1:00 in the left. OCT imaging confirmed that both eyes showed pupillary block, and the left eye demonstrated severe angle narrowing.
The patient was treated initially with 250mg of Diamox (acetazolamide, Duramed Pharmaceuticals) and one drop of Lumigan (bimatoprost ophthalmic solution 0.01%, Allergan) and Combigan (brimonidine tartrate/timolol maleate ophthalmic solution 0.02%/0.05%, Allergan) to reduce IOP to 38mm Hg. Attending doctors achieved further reduction in IOP to 15mm Hg using compression pressure with a four-mirror gonio lens. The posterior force of the gonio lens mechanically opened the iridocorneal angle, resulting in rapid lowering of IOP.
The patient was instructed to continue using Lumigan QHS OS, Combigan BID OS, and Diamox Sequels 500mg (acetazolamide ER, Duramed Pharmaceuticals) PO BID in addition to her postsurgical drops, until a follow-up could be scheduled in four days with her surgeon. The surgeon agreed with the proposed treatment plan, and scheduled an ICL exchange with a shorter lens upon her return.
1. Chun YS, Park IK, Lee HI, et al. Iris and trabecular meshwork pigment changes after posterior chamber phakic intraocular lens implantation. J Cataract Refract Surg. 2006 Sep;32(9):1452-8.2. Choi KH, Chung SE, Chung TY, Chung ES. Ultrasound biomicroscopy for determining visian implantable contact lens length in phakic IOL implantation. J Refract Surg. 2007. Apr;23(4):362-7.
