The concept of dry eye, or at least an understanding of the need for tears, has been recognized by healers for over 3,500 years, as the first mention of our tears was recorded in 1550 BC as “the water within” in ancient Egyptian documents known as the Ebers Papyrus.1 However, the discipline of ocular surface care didn’t actually begin until the mid-1850s, when a mechanism of tear secretion was first proposed. The modern era of dry eye began in 1973 when Frank Holly explained the role of mucin. Soon thereafter, the work of Tseng, Plugfelder, Lemp, Korb, Nichols and others allowed us to develop a better understanding of the interaction of the ocular surface and tear film.
| |
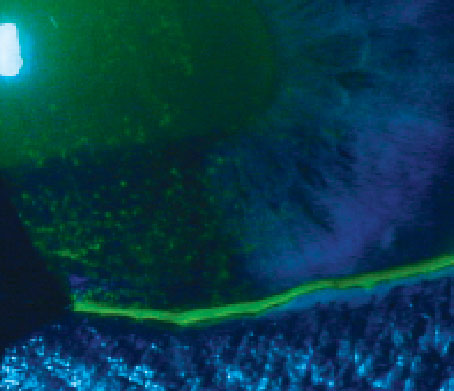
| Dry eye in a patient who presented with superficial punctate keratitis. |
Today, dry eye is one of the leading causes of patient visits to eye care providers (ECPs) in the US.3 Although anywhere from 20 to 30 million people have early signs and symptoms of dry eye (depending on the study cited), only eight million patients manage their condition with artificial tears at a minimum, and a much lower percentage are actually receiving ongoing treatment from an ECP.4 Studies around the world show similar numbers, though certain regions like Asia may have as much as 33% of the population experiencing significant dry eye.2
Simply put, dry eye is the number one medical condition that motivates patients to see their ECP—and it will only grow. The predisposing factors that will likely make this disease increase in prevalence are:
• Digital device use. Studies show the average American spends three to five hours on electronic devices daily.5
• Systemic diseases
. Diabetes is just one example of a systemic disease with a significant connection to dry eye; it is expected to increase from 29 million Americans in 2012 to 54 million in 2050.6,7
• The aging population
. Demographic trends and life expectancy gains will expand the senior citizen population from 14% in 2013 to 20% in 2050.8
These trends—which clearly indicate a pressing need for ongoing education in the field of dry eye—are the impetus for this new bimonthly column, “Ocular Surface Review.”
Past Meets Present
Along the historic path, there were some great, early insights that impact how the disease is diagnosed and managed today.
The first mention of increased tear osmolarity was in 1941 by Von Bahr and colleagues.9 But osmolarity requires two key things: acquisition of tears in a reservoir, and then measurement. Although those capabilities were not as readily available then as they are today, the science of hyperosmolarity as an underlying finding began almost 75 years ago.
In the early 1960s, it was discovered that a decrease in lacrimal gland secretion leads to ocular surface desiccation.10 In the 1970s, the multilayered ocular surface was recognized as an integrated functional unit. This is analogous to our present efforts to consider the conjunctiva, cornea, lacrimal and meibomian glands as interrelated parts of a functional anatomical unit.
The late 1970s brought us the first mention of the role of meibomian glands in the pathogenesis of evaporative tear loss, and the role of the lipid layer in preventing the loss of aqueous was identified soon afterward.10,11 These clinical findings have affected how we manage dry eye disease and play a key role in the tests and treatments being administered.
Despite our knowledge today, there is no “gold standard” for the diagnosis of dry eye disease; instead, we must interpret multiple testing results. This fundamental piece of the dry eye puzzle is similar to the management of glaucoma, where many objective and subjective factors play a part in revealing the evidence that helps determine the diagnosis.
The combination of these as well as other key findings—like MMP-9, blink analysis, eyelid apposition and symptomatology—all provide the data we need to diagnose dry eye.
Part of the reason we have to employ multiple tests in the diagnosis is because signs and symptoms of DED are poorly correlated.12,13 In fact, many patients with significant symptoms may have milder forms of dry eye. As the nerves downregulate and signs become more apparent, the symptoms decrease. In fact, one study showed less than 60% of dry eye patients (based on objective signs) were actually symptomatic.14
The progressive nature of this disease also increases the importance of recording objective findings like meibography, osmolarity, MG expression, inflammatory marker testing, lid margin evaluation, vital dye staining, blink analysis and lid apposition.15
With this many factors to continually monitor and evaluate, modern dry eye care can seem daunting. Fortunately, a few recent studies are helping to connect the dots.
One recent paper found that variability between eyes in osmolarity testing is a hallmark sign of DED. For example, the difference in osmolarity readings between the eyes would be within 5mOsmol/L, and both eyes would have readings under 300mOsmol/L.
A second critical new finding, also published in late 2014, mapped the inflammatory cascade. The sequence is as follows: increased osmolarity ’ inflammation ’ tear film instability ’ rapid tear film break-up time ’ change in VA ’ eventually other symptoms and signs.
Another landmark study looked at the effect of desiccating stress on the mouse meibomian gland function.16 The proposed cascade is as follows: low humidity ’ chronic evaporative stress ’ increased meibocyte production > oil production ’ dilation of ducts, extensive and possible obstruction ’ short maturation time = increase in protein/lipid ratio ’ tear film stability impaired equal to or greater than evaporative stress.
All of these studies were published in 2014 and will have major implications to how we manage dry eye going forward. They also have significant areas of overlap, even though the original cause may be different.
Routine Check-ups
Given the progression of this disease, one might surmise the most appropriate future protocol might be that of the dental model. In this analogy, patients—especially those with early symptoms such as end-of-day contact lens discomfort or decreased wear time—should be evaluated and managed routinely, even in the absence of symptoms, to prevent future damage or loss of glands.
In the 1850s, when dry eye research began, people didn’t know to brush their teeth, and they eventually lost them. Today, because of the use of electronic devices in particular, patients are losing their meibomian glands. We should be assessing this every year at a minimum and suggest that patients manage the early disease before it progresses.
Our eyelids are like our gums—they need to be managed daily. Patient education should stress the importance of daily at-home care with lid wipes and warm compresses. In the office, we can offer thermal pulsation treatment, mechanical cleaning devices that remove biofilms and debridement/scaling of the lid margin. When the lids are inflamed, we may need to use medications like topical cyclosporine or corticosteroids, and in advanced cases, orals like doxycycline.
We must embrace this new understanding of OSD to help our patients live with the most common condition they will face for decades to come. Working to shorten the adoption lifecycle will have an amazing effect not only on dry eye disease patients and more advanced forms like Sjögren’s syndrome, but also contact lens wearers, those who use electronic devices more than three hours a day and patients preparing for procedures such as cataract surgery. Getting involved now will help your practice and, most importantly, your patients’ quality of life. n
Excerpts taken from the Dry Eye Summit, which took place on December 12, 2014 in Dallas/Fort Worth, with input from 30 of the top educators in ocular surface disease.
1. Hirschberg J. The History of Ophthalmology, Vol. 1: Antiquity. Translated by FC Blodi. Bonn, West Germany: Verlag JP Wayenborgh, 1982.
2. Gayton, JL. Etiology, prevalence, and treatment of dry eye disease. Clin Ophthalmol. 2009; 3: 405–412.
3. Sullivan, D.A., Hammitt, K.M., Schaumberg, D.A. et al. Report of the TFOS/ARVO Symposium on Global Treatments for Dry Eye Disease: An unmet need. Ocul Surf. 2012; 10: 108–116
4. Dahl AA and Davis CP. Dry Eye Syndrome (Dry Eyes, Keratoconjunctivitis Sicca).
Available at: www.medicinenet.com/dry_eyes/article.htm. Accessed September 19, 2014.
5. U.S. Dept of Labor. American Time Use Survey Summary. Available at: www.bls.gov/news.release/atus.nr0.htm. Accessed October 1, 2014.
6. Centers for Disease Control and Prevention. National Diabetes Statistics Report, 2014. Available at: www.cdc.gov/diabetes/pubs/statsreport14/national-diabetes-report-web.pdf. Accessed October 1, 2014.
7. Centers for Disease Control and Prevention. Number of Americans with Diabetes Projected to Double or Triple by 2050. Available at: www.cdc.gov/media/pressrel/2010/r101022.html. Accessed October 1, 2014.
8. Ortman JM, Howard H, Victoria VA. An Aging Nation: The Older Population in the United States. May 2014. Available at: www.census.gov/prod/2014pubs/p25-114.pdf. Accessed October 1, 2014.
9. Von Bahr G. Konnte der Flussigkeitsabgang durch die cornea von physiologischer bedengtung sein. Acta Ophthalmol (Copenh). 1941;19:125-34.
10. Asbell PA, Lemp MA (eds.). Dry Eye Disease: The Clinician’s Guide to Diagnosis and Treatment. Thieme Publications; 2006
11. Jester JV, Nicolaides N, Smith RE. Meibomian gland studies: histologic and ultrastructural investigations. Invest Ophthalmol Vis Sci. 1981;20:537-47
12. Nichols KK, Nichols JJ, Mitchell GL. The lack of association between signs and symptoms in patients with dry eye disease. Cornea. 2004 Nov;23(8):762-70.
13. Sullivan BD, Crews LA, Messmer EM, et al. Correlations between commonly used objective signs and symptoms for the diagnosis of dry eye disease: clinical implications Acta Ophthalmol. 2014;92:161-166.
14. Bron AJ, Tomlinson A, Foulks GN, et al. Rethinking dry eye disease: a perspective on clinical implications. OculSurf. 2014;12(2 Suppl):S1-S31.
15. Rao SN. Topical cyclosporine 0.05% for the prevention of dry eye disease progression. J Ocul Pharmacol Ther. 2010 Apr;26(2):157-64.
16. Suhalim JL, Parfitt GJ, Xie Y, et al. Effect of desiccating stress on mouse meibomian gland function. Ocular Surface 2014, Vol. 12 (1):59-68.
