|
|
 |
Human immunodeficiency virus (HIV) is a blood-borne retrovirus. Acquired immune-deficiency syndrome (AIDS) is caused by HIV and is characterized by profound immune suppression that leads to opportunistic infections (OIs), secondary neoplasms, neurological manifestations and possible death.
In the United States, HIV was first described in 1981 among two groups, one in San Francisco and the other in New York. Numerous young homosexual men presented with opportunistic infections that were typically associated with severe immune deficiency: Pneumocystis pneumonia (PCP) and aggressive Kaposi sarcoma.1 HIV itself was not identified for another two years.2
People at Risk
Men who have sex with men continue to bear the greatest burden of infection. Among races/ethnicities, African Americans and Hispanic/Latinos are disproportionately affected, as are injection drug users.3,4
People with sexually-transmitted diseases (STDs) often also have, or are more likely to get, HIV.4,5
Transmission
and Transcription
HIV is typically transmitted via sexual intercourse, shared intravenous drug paraphernalia and mother-to-child transmission, which can occur during birth or breastfeeding. HIV disease is caused by infection with HIV-1 or HIV-2, which are retroviruses in the Retroviridae
family, Lentivirus
genus.
|
|
|
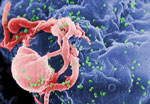
This scanning electron micrograph shows HIV-1 budding from a cultured lymphocyte. Image: CDC/C. Goldsmith
|
|
Retroviruses use RNA as their genetic material, but the host cell must synthesize a “DNA copy” of the RNA before it can be transcribed or translated. This task is aided by the action of an enzyme known as reverse transcriptase.6
Like others in the lentiviral genus, HIV creates a long interval between initial infection and serious symptoms. It targets the immune system by primarily affecting an arm of adaptive immunity called “cell-mediated immunity.”
The cluster of differentiation 4 (CD4) molecule, found on T helper (Th) and other immune system cells, is a high-affinity receptor for HIV. Binding to CD4 is not sufficient for infection, so HIV must also bind to other surface molecules for entry. Mature Th cells that express CD4 (CD4+T cells), along with macrophages and follicular dendritic cells contained in lymphoid tissues, are the major sites for HIV infection and persistence.7
Clinical Signs
Viral replication occurs in the regional lymph nodes and leads to viremia with eventual seeding of lymphoid tissue. Acute retroviral syndrome, the initial response to HIV infection, occurs approximately four weeks after infection. Clinically, this phase is a self-limited acute illness with flu-like symptoms such as rash, sore throat, vomiting, myalgias, fever, weight loss and fatigue.
The following chronic stage may last for several years. The patient may be asymptomatic, but generalized lymphadenopathy, thrush, herpes zoster and thrombocytopenia may be noted during this time. Activation of CD8+ cytotoxic T cells appears to be the primary mechanism for immunologic control of HIV. T cell responses are correlated with the steady-state viral load and thus the rate of progression.5,7
The final phase is progression to AIDS. In the United States, a CD4+T cell count less than 200/µL is used as a measure to diagnose AIDS. Long-lasting fever, fatigue, weight loss and diarrhea may occur, as well as OIs, secondary neoplasms and neurological disease. These account for the majority of deaths in patients with AIDS.2,7
|
|
The Eye and HIV
|
A high-sensitivity enzyme-linked immunoabsorbent assay (ELISA) should be used for screening; a positive result should be followed with confirmatory testing. The CD4+T cell count reliably reflects the current risk of acquiring OIs. Viral load in peripheral blood is used as a surrogate marker of viral replication rate. Patients with viral loads greater than 30,000/µL are 18.5 times more likely to die of AIDS than those with undetectable viral loads.7
Antiretroviral Treatment
The use of combination antiretro-viral therapies and prophylaxis for IOs dramatically improves survival.7,8
The US Food and Drug Administration has approved a once-daily, fixed-dose triple-combination pill (Triumeq, ViiV Healthcare) containing the antivirals dolutegravir, abacavir and lamivudine for the treatment of patients aged 18 years or older. Overall, with the increasing use of antiretroviral therapy and the introduction of better regimens, survival with HIV has increased.
Society has made substantial progress, but we continue to face challenges. Patients with HIV should be counseled on the risks of infecting sexual partners. Safe sex practices and treatment of STDs, in the patient and sexual partners, considerably reduces the risk of transmission. Intravenous drug users should be counseled on the risks of sharing paraphernalia.
Ocular Complications
Approximately 80% of HIV-infected patients will be treated for an HIV-associated eye disorder.9
The optometrist may be presented with adnexal, anterior segment, posterior segment or orbital manifestations. Adnexal manifestations may include herpes zoster or conjunctival microvasculopathy, among others. Anterior segment findings include tumors of the periocular tissues and a variety of external infections. Posterior segment changes include an HIV-associated retinopathy/vasculopathy and a number of OIs of the retina and choroid. Orbital manifestations of HIV are rare; however, the most common complications include orbital lymphoma and orbital cellulitis due to Aspergillus
infection.9
|

|
|
|
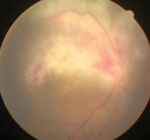
Cytomegalovirus retinitis in a patient with AIDS.
|
HIV retinopathy may present with cotton-wool spots and vascular changes. |
|
Increasing longevity of individuals with HIV may result in greater numbers of patients with ocular complications. Fortunately, many of these are now treatable. Partial immune system recovery following initiation of effective antiretroviral therapy may modify clinical presentation of OI and can affect response to treatment. In addition, several infections may occur in a single eye at the same time, rendering diagnosis and therapeutic intervention more difficult.
Due to the potentially devastating and rapid course of OI, patients with HIV should undergo regular evaluations. With early-stage HIV, ocular syndromes associated with immunosuppression are uncommon. Nonetheless, ocular infections associated with STDs may be more frequent in patients with HIV; therefore, clinicians should screen for HIV in the presence of these infections.
1. Friedman-Kien A, Laubenstein L, Marmor M, et al. Kaposi’s sarcoma and Pneumocystis pneumonia among homosexual men—New York City and California. MMWR Morb Mortal Wkly Rep. 1981;30(25):305-8.2. Barre-Sinoussi F, Chermann JC, Rey F, et al. Isolation of a T-lymphotropic retrovirus from a patient at risk for acquired immune deficiency syndrome (AIDS). Science. 1983;220(4599):868-71.
3. CDC. Monitoring selected national HIV prevention and care objectives by using HIV surveillance data—United States and 6 dependent areas—2012. HIV Surveillance Supplemental Report. 2014;19(3).
4. CDC. Estimated HIV incidence in the United States, 2007–2010. HIV Surveillance Supplemental Report. 2012;17(4).
5. CDC. HIV Surveillance Report. 2012;24.
6. Carter J, Saunders V. Virology: Principles and Applications (Paperback). 2013:1-65.
7. Kumar V, Abbas A, Fausto N. Robbins and Cotran Pathologic Basis of Disease, 7th ed. Philadelphia: Elsevier Saunders; 2005:245-258.
8. Hirsch DA, Jones S, Wallach F, et al. Ocular manifestations in individuals infected with the human immunodeficiency virus. Comprehensive Ophthalmology Update. 2004;5(1)3-14.
9. Copeland Jr R, Phillpotts B. Ocular Manifestations of HIV Infection. http://emedicine.medscape.com/article/1216172-overview#aw2aab6b5.
