| |
|
| Vol. 2, #12 • Monday, June 7, 2021 |
|
|
|
|
| |
|
Review's Chief Clinical Editor
Paul M. Karpecki, OD, FAAO
Provides you with cutting-edge clinical strategies for optimal management of ocular surface disease and beyond.
|
|
|
|
|
|
Dry eye disease diagnosis doesn’t have to be complicated but it goes beyond the finding of symptomatic eye dryness.
I’ve heard it said that dry eye disease is easy to diagnose because if the patient complains of dry eyes you have your answer. I wish it were that easy but unfortunately, DED is a far more complex and multifactorial condition than such a simple conclusion would allow.
Though dry eye disease does require signs to go along with symptoms, it can still be easy to manage. So do take into account complaints of dry, gritty or burning eyes, but confirm the diagnosis with signs such as osmolarity, ocular surface staining, tear film break-up time, tear meniscus height, or meibomian gland expression. Diagnostics can be efficient, and here are three tests to consider:
Osmolarity Testing: While I don’t think it’s necessary to have osmolarity when you are starting a dry eye clinic, I do believe it’s a necessity if you plan to specialize in dry eye. It’s a five-second test and has the highest predictive value of any diagnostic test available.1,2 Readings over 308mOsmol/L in either eye indicate DED, and a difference of more than 6mOsmol/L between eyes indicates tear film instability.
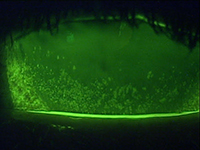
Ocular Surface Staining: If you are looking for a single test to measure dry eye, this may be a good choice given the fact that you have four tests in one. Once NaFl dye is instilled in the eyes, wait about a minute for it to equilibrate with the tears. The four items to observe include punctate corneal staining, punctate conjunctival staining (may require a Wratten filter), tear film break-up time, and tear meniscus height. All factors are valuable to evaluate and become more evident with dye.
Meibomian Gland Expression: This five to 10-second test of the lower nasal to central eyelids is especially important in deterring evaporative DED. A thin and clear oil expression is normal, while turbid, thickened, paste-like or non-expressive findings indicate meibomian gland dysfunction and potential evaporative DED.
|
|
|
|
KEY TAKEAWAY: Since a sign is needed along with symptoms to confirm dry eye disease, consider one or more quick and easy diagnostic tests including osmolarity, ocular surface staining, and meibomian gland expression.
1. Keech A, Senchyna M, Sullivan BD, et al. Impact of time between collection on human tear film fluid osmolarity. Invest Ophthalmol Vis Sci. 2010;51:E-Abstract 4174.
2. Sullivan BD, Eldridge DC, Berg M, et al. Diagnostic performance of osmolarity combined with sub-set markers of dry eye disease in an unstratified patient population. Invest Ophthalmol Vis Sci. 2010;51. ARVO E-Abstract 3380.
|
|
|
|
| Supported by an independent medical grant from Kala Pharmaceuticals |
|
| |
| |
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 19 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|
|
|
|
|
|
|
|