| |
|
| Vol. 2, #16 • Thursday, July 15, 2021 |
|
|
|
|
| |
|
Review's Chief Clinical Editor
Paul M. Karpecki, OD, FAAO
Provides you with cutting-edge clinical strategies for optimal management of ocular surface disease and beyond.
|
|
|
|
|
|
|
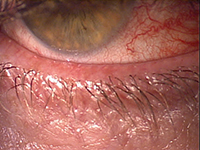
| Conjunctival injection is a key sign of inflammation. |
The key to suppressing DED's inflammatory response is with a corticosteroid.
Immune-mediated diseases such as dry eye follow a similar pattern involving periodic flareups. Other conditions such as asthma, atopic dermatitis, rheumatoid arthritis, and various autoimmune diseases are also known for periodic flares. Asthma, in particular, is a chronic condition in which inflammatory episodes result in edema and narrowing of the bronchial pathways with increased production of mucin. Asthmatic flares are best treated with steroid inhalers.
Along similar lines, inflammation of the ocular surface plays a key role in acute cases of dry eye. I know many patients (including myself) who experience episodic dry eye flares after a long flight, for example. Rather than turning to long-term immunomodulators, I have found that a short course of steroid drops quiets the flare rapidly and completely.
Flareups also tend to occur in patients with chronic DED who rely on immunomodulators. This is especially apparent during allergy season or during the cold, dry winter months. It is estimated that 91% of patients on long-term therapy experience four to six flares per year.1,2
The pathophysiology of dry eye begins with hyperosmolarity that results in ocular surface inflammation. This activates immune cells that migrate to the lymph nodes, triggering an autoimmune response. Immune cells travel from the lymph nodes to the ocular surface to perpetuate the cycle of inflammation. The system is based on innate vs. adaptive immunity. An innate response is an immediate, nonspecific response, which can evolve into an adaptive response (a specific, autoimmune response) as it increases in frequency or in response to a specific stimulus. In adaptive immunity, T-cells become primed, resulting in a programmed response that is more severe and long-lasting.
Clinically, this phenomenon manifests as dry eye symptoms—in particular, conjunctival hyperemia—that patients cannot control. In fact, the hallmark sign of inflammation is present in many ocular conditions including DED.
In the case of DED flares, EYSUVIS (0.25% loteprednol) can be prescribed QID for up to two weeks. That is typically more than enough time to suppress the dry eye flare.
|
|
|
|
KEY TAKEAWAY: Immune-mediated diseases like dry eye and asthma are prone to flareups. The best way to quickly and effectively suppress an inflammatory response is with a corticosteroid. The recent FDA approval of EYSUVIS for the short-term treatment of signs and symptoms of DED is welcome, and validates how dry eye should effectively be managed.
1. 2020 Study of Dry Eye Sufferers. Multi-sponsor Surveys, Inc. July 2020.
2. Brazzell RK, Zickl L, Farrelly J, et al. Prevalence and characteristics of dry eye flares: a patient questionnaire survey. Presented at: AAO 2019: October 12-15, 2019; San Francisco, CA.
|
|
|
|
| Supported by an independent medical grant from Kala Pharmaceuticals |
|
| |
| |
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 19 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|
|
|
|
|
|
|
|