|
More than 20 years ago, when I first dedicated a significant portion of my clinic to DED management, I would typically treat a patient once I confirmed a diagnosis via NaFl corneal staining. Of the three grades of DED most commonly encountered by an optometrist, the presence of confluent, macropunctate or central staining is indicative of the most clinically severe level. This approach, in essence, was equivalent to waiting for a glaucoma patient to exhibit a 0.8 x 0.8 cup-to-disc ratio and demonstrate visual field loss before starting treatment. Today, no eye care professional should manage dry eye patients in such a conservative capacity.
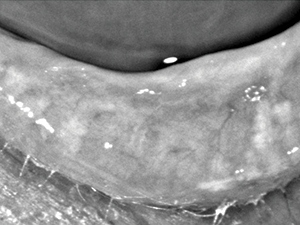
The most frequently overlooked form of DED is evaporative dry eye. Meibomian gland dysfunction (MGD) is the most common risk factor for this type of disease. Thus, clinicians must identify the presence of MGD or blepharitis. This involves meibomian gland expression, as well as other sensitive tests, such as meibography, to determine compromise. Expression may include digital manipulation, use of a wet Q-tip behind the eyelid, or an instrument such as a Mastrota paddle (OcuSoft) or MG Evaluator (TearScience).
Research by Donald R. Korb, OD, shows that the majority of tear film oil emanates from the lower eyelid—specifically the lower nasal and central eyelids.2 Expression includes pushing on these glands and monitoring ease of expression, and whether the discharge is clear, turbid, thickened, gelatinous or paste-like, or if it is non-expressible.
Once you know MGD is present, the next step is to determine if the tear film can maintain homeostasis. Tests such as tear film osmolarity, non-invasive tear film break-up time and patient symptom questionnaires all can assist in confirming evaporative DED, and suggest prompt intervention.
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017 Jul;15(3):276-283.
2. Korb DR, Blackie CA. Meibomian gland diagnostic expressibility: correlation with dry eye symptoms and gland location. Cornea. 2008 Dec;27(10):1142-7.
.

|