 Q: A patient presented to my office five days after getting a piece of metal in his eye. The foreign body was central and seemed deep, so I referred the patient out. Was that the right move?
Q: A patient presented to my office five days after getting a piece of metal in his eye. The foreign body was central and seemed deep, so I referred the patient out. Was that the right move?
A: There are several reasons why the O.D. might refer out a patient with a foreign body (FB). But, usually these are also the same reasons why we should seize the opportunity to remove the foreign body ourselves:
- The foreign body is central and might leave a scar. If the FB is going to leave a scar, it’s going to leave a scar no matter who removes it. So the sooner you get it out, the better.
- The patient is in pain. If so, that’s a good reason to remove it right away so that the cause of the pain will be eliminated.
- The foreign body appears deep. Many FBs that appear deep are no deeper than the epithelium or anterior stroma. But even if it’s in the deep stroma, you can usually take the FB out yourself, as long as you do it properly. Here’s how to do it:
1. Anesthetize the eye. Use proparacaine or, if the patient is very sensitive or the FB is at the limbus, consider using Akten (lidocaine 3.5%, Akorn Inc.), an ophthalmic gel that provides deeper anesthesia.
2. Identify the foreign body. While a lot of the FBs we see are metallic, don’t assume this one is. But, even if it is an unusual object—such as bugs’ wings, spatters of latex paint, droplets of Super Glue, or just an unidentified foreign body—that in itself shouldn’t prompt you to refer the patient.
Some doctors advocate allowing rust to remain for a few days to allow it to “rise to the surface” or “soften up.” I disagree. The longer rust remains in the cornea, the more likely it will cause an immune response. We’ve actually seen an immune ring that formed around a FB and started to thin the cornea. So, no matter what the foreign body is, including rust, just get it out.
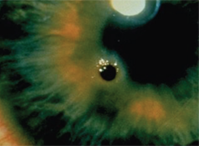
Corneal foreign body with rust ring.
3. Use the proper tools. You’ll need a pair of jeweler’s forceps, a foreign body spud (like a golf club spud) and an Alger brush.
Focus your attention first on removing the object (using the spud), and worry about the rust after the FB is out. (You don’t want to start with the Alger brush and turn one piece of metal into a million fragments, when you could have taken it out in one piece.)
If there is rust left behind, nothing gets it out better than an Alger brush. Place the instrument right on the edge of the crater and apply pressure to clean out the area. Don’t worry; if you push too hard or too deep, the drill motor will stop on its own.
4. Make sure it’s all gone. With any FB, make sure to evert the upper and lower lids. We occasionally see what’s described as an “infectious ulcer,” which is really a FB abrasion caused by an embedded lash or hidden foreign body in the upper or lower lid.
5. Prevent infection and pain. We no longer patch eyes, even those with large FBs or abrasions. So, to prevent infection of the open epithelial defect, prescribe a short course (up to seven days) of a topical antibiotic. To take the edge off the pain, prescribe a topical NSAID. For patients in severe pain, be prepared to prescribe an oral narcotic analgesic. Copious artificial tears also help with comfort and healing.
6. Be on call. Be available after hours for these patients. Give them your cellphone number or some way to reach you directly if there’s a problem. Telling patients to go to an emergency room after hours is a recipe for disaster—and a lawsuit.
7. Follow up in 24 hours. Have the patient come back the next day so you can check the eye’s condition. Also, use this as an opportunity to educate the patient about the importance of protective eyewear.
Also, don’t forget to document everything in the patient’s chart—what you did, what instructions you provided, and any precautions you gave for the future. Last but not least, if you have any suspicion that the FB caused a penetrating injury, perform gonioscopy and dilation. If it does appear to have penetrated, get an X-ray of the eye.
