More than 20% of patients age 45 and older report dry eye or its symptoms.1 But, a survey of diagnostic and treatment practices indicates that most eye care providers manage these signs and symptoms based only on clinical findings.
This same survey found agreement among practitioners that dry eye is complex and that its etiology and treatment are multifactorial. So, why would we only utilize one small base of information rather than look at the whole picture of the patients history and address the underlying causative factors?
Dry eye treatment conducted in isolation is often doomed to failure. We must look at the whole patient rather than an individual part. The best solutions result from considering multiple causal factors rather than by treating a specific symptom or only one part of the underlying problem.
We suggest a whole-istic approach that investigates all known factors to develop a
system for prescribing treatment.
This starts with an independent dry eye evaluation.1 The number of underlying factors can only be discovered by an orchestrated comprehensive assessment, including age, gender, systemic health, family history, prescription and over-the-counter (OTC) medications, nutrition, vocational and avocational activities, and environmental factors.
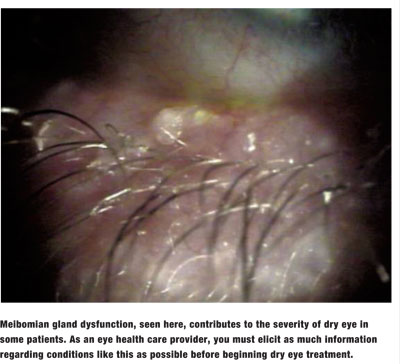
Each of these may contribute to the patients condition. A battery of clinical measures and an assessment of the severity of the patients condition should then complement the patients history.2,3
Systemic History
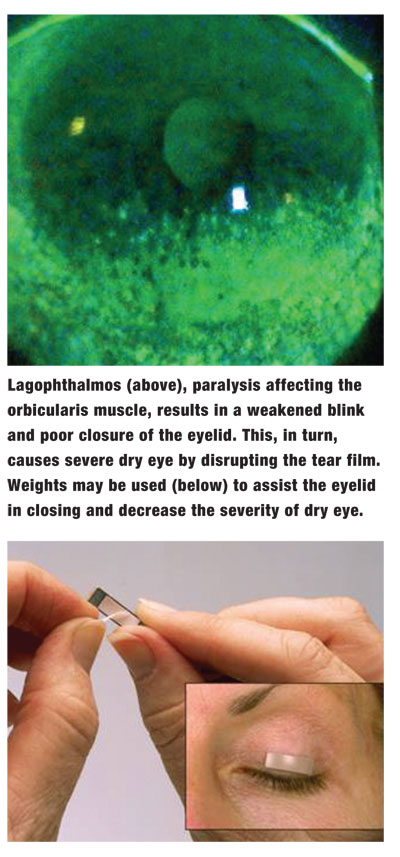
Your systemic health assessment for dry eye must elicit as much information as possible about previous surgeries, endocrine system anomalies, sleep disorders and allergy. For example, you might treat a patient for weeks before he casually volunteers that he has sleep apnea, which is associated with dry eye. You thought you had asked the right questions to elicit the disorder; however, it was not reported to you.
One possible solution: Make a comprehensive questionnaire with a methodical approach to systemic health problems that are factors in dry eye.
Family History
Dry eye questionnaires should also probe relevant factors of family history. Both nature and nurture are, in a sense, inherited, and will play a role in the management of your patients. Family history can provide an understanding of genetic and lifestyle patterns that may contribute to dry eye. For example, patients who present complaining of excessive dryness need to be questioned about autoimmune conditions, such as rheumatoid arthritis, systemic lupus erythematosus, fibromyalgia, rosacea, Sjgrens syndrome and Stevens-Johnson syndrome. These conditions can lead to significant dry eye.4 Also, the drugs used to treat them may exacerbate the patients condition.5 (For more on these, see The Inside Track on the Bodys Attack.")
Most of these conditions are hereditary. If your patient history does not investigate all aspects of potential problems, you will only be looking at the dry eye problem in isolation, not in context.
Medications
Dry eye is a side effect of many common medications. So, youll need to ask what medications patients currently take and have used in the last five years. Patients usually reveal what prescription medicines they are taking but may not mention their use of OTC medications.
Your questionnaire must explore the use of key OTC and prescription medications. Patients often do not understand the importance of you knowing about these agents. So, a female patient may not reveal her use of hormone replacement therapy (HRT) due to embarrassment, yet HRT plays a role in dry eye symptoms and management. Or, patients may not disclose use of oral contraceptives (especially younger patients) or OTC hormones that are available in health food stores.
Interestingly, the establishment of a formal dry eye evaluation raises the importance of gathering information from your patients. As a result, more necessary information may surface in their responses to you.
When asking about OTC agents, ask about vitamins. Though many patients take vitamins today, you cannot just assume that they take multivitamins; they may be taking specific doses of non-traditional vitamins for a given purpose that they never relate to their eyes directly. Vitamins associated with dry eye include antioxidants, vitamin C and many forms of specific vitamins marketed as ocular vitamins.
Unless you know the specifics about all their prescription and OTC medicines, you cannot help patients ascertain if what they take affects their normal tear mechanisms. But, be careful and nonjudgmental in your approach. If a patient thinks you are displeased with his self-modulated medicinal regimen, he will volunteer as little as possible.
Nutritional Habits
The relationship between dry eye and nutrition is only partially understood. However, a complete history of your patients dietary trendsplus alcohol and tobacco usecan help establish a possible cause of the patients dry eye symptoms and may suggest the need for your patients to modify their diets.5 Also, the formal dry eye evaluation educates patients about the significance of these factors.
Measurement is the first step to modulation. A comprehensive nutritional questionnaire as part of the formal dry eye evaluation will provide information for an intelligent system of treatment.
Patients whose diet is lacking in fish and other key food groups may have a deficiency in omega fatty acids; this deficiency contributes to their dry eye problems.6 Modulation of diet is generally part of an effective treatment regimen for dry eye therapy. Sometimes, though, the addition of omega-3, -6 and/or -9 fatty acids is not enough to erase a patients dry eye condition. In such cases, the patient should supplement his diet with other nutraceuticals, such as evening primrose seed or liquid flaxseed oil.
Concentrated Visual Tasks
The Information Age brought with it a significant challenge to the ocular surface. The reduced blink quantity and the change in the quality of the blink with concentration may be the single greatest contributor to dry eye.1,7 The vocational and avocational assessment you give your patients must explore their amount of computer use and their reasons. Computer use with performance demands may be more significant than casual use.
Ask about daily activities in and out of the workplace that may play a role in dry eye. The number of hours at the computer, driving, or watching television or movies should be known along with outdoor activities in windy and sunny conditions. Since squinting interrupts blinking, find out if the patient uses eyewear for sun and wind protection, or if he or she has a pattern of squinting.
The Environment
You must consider environmental factors when treating dry eye. A useful questionnaire should explore the presence of noxious fumes, dust, mold and mildew, and your patients need to understand the role that these play in dry eye. Household pets and the foliage in and around the residence and workplace also are factors in dry eye.
How your patients clean their air-conditioning filters and heaters and the age of these systems may also affect the ocular surface. As the filters in heating and cooling systems clog with particles, the pressure from the system sometimes breaks these particles into micro-dust and pushes it through the filter. If this dust is a potent antigen or ocular irritant, it will affect your patients eyes adversely, either as an allergen or an ocular surface disease.
It may be difficult to differentiate between true dry eye and an allergic reaction. The difference is critical, though, because the necessary treatment generally varies. For example, if one individual lives at a high altitude, where the air is thin and the humidity is low, while another lives at sea level, where the air is thicker and the humidity is high, there will be distinct differences in how the particulates in the air affect each of them.
Also, depending upon the pollutants in the air both outside and inside their particular environments, one individual may be more subject to allergic problems, and the other may be subject to pure dryness problems. The symptoms, however, may be the same. A good dry eye questionnaire can help differentiate these two contributing conditions.
The Dry Eye Clinical Assessment
A comprehensive dry eye clinical assessment goes beyond the standard comprehensive examination. The assessment should start with non-invasive testing and proceed to invasive tests. As a starting point, we suggest measuring blink quality and quantity without making the patient aware of this observation. It may be useful to repeat this measure while having the patient complete a task at a computer terminal that has a timed performance test.
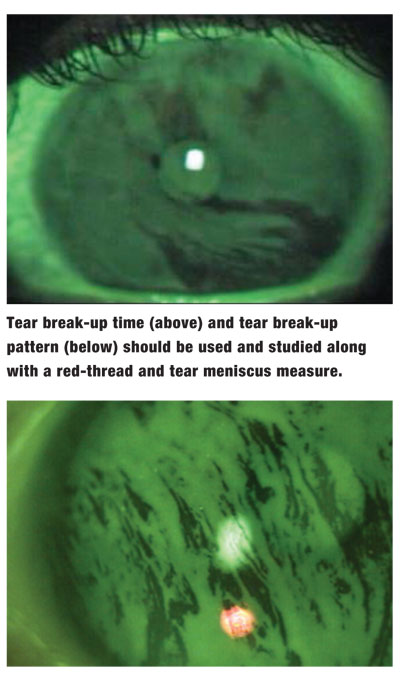
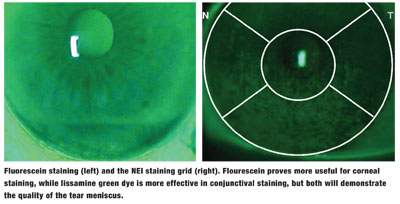
Tear break-up time (TBUT) and tear break-up pattern should complement a red-thread and tear meniscus measure. In addition, fluorescein staining following the TBUT evaluation and lissamine green staining should be conducted along with appropriate assays of tear chemistry. Fluorescein staining has been shown to be more useful for corneal staining, while the lissamine green dye is more useful for conjunctival staining.8
Low tear meniscus is a significant clinical indicator of dry eye.
Debility Assessment
A distinction between illness and disease may be useful. One can have disease without illness and illness without disease. You must determine your patients degree of illness.
In other words, the patient may have clinical signs of ocular surface disease without any symptoms or complaints (illness), or he or she may suffer illness with no apparent disease. There is value in finding the relationship between the symptoms and reported debility, the clinical signs and the antecedents or precursors.
Dry eye management commonly includes environmental engineering or a change of habits. An assessment of the degree of suffering and debility will discover the foundation for patients motivation to follow through on a treatment plan that requires effort on their part. Patients that have disease without illness are far less likely to make changes.
Evidence-Based Treatment
Treatment of the patient is then based on the assessment. The history and clinical assessment provides the evidence for a whole- istic treatment plan. While the plan may include punctal or lacrimal plugs and ocular lubricants, it may also include recommendations for environmental changes, cues for increasing blink quantity and techniques for improving blink quality during concentrated visual tasks, changes in nutrition or the addition of nutritional supplements.
Action Plan to Develop Your Dry Eye Practice 1. Establish a dry eye evaluation procedure for your practice. 2. Expand the systemic health history. 3. Look at the role of family history. 4. Ask about all prescribed and OTC medications used. 5. Implement a thorough nutritional questionnaire. 6. Ask about vocational and avocational activities. 7. Discuss pertinent environmental factors. 8. Implement a comprehensive battery of clinical tests. 9. Discover the degree of suffering and debility from the disease. 10. Provide an all-inclusive assessment-based treatment plan. 11. Learn and implement appropriate coding and billing for treating dry eye.
Dry eye management is one of many areas in which the optometrist may be an advocate for the patient with his or her other health-care providers. This is particularly true when systemic medications appear to play a role in the disease process. For example, the allergy patient who is undergoing sensitization (shot) therapy with an allergist and simultaneously taking a daily antihistamine or decongestant may have concomitant dry eye. Then, the O.D. must work with the allergist to develop a treatment plan that balances both objectives, namely allergy relief and relief of dry eye, and prevents any new symptoms coming about from the existing treatment.
Another example: a patient whose physician prescribed selective serotonin reuptake inhibitor (SSRI) medications for anxiety or depression. These drugs are known to exacerbate dry eye and, in some cases, may actually cause dryness. In this case, your patient may present during any stage of the therapy from before the drug is prescribed to several months or years after the course of this medication. Unless you investigate thoroughly, you may not discover the source of the patients dry eye. That means you may think of it as an isolated entity rather than a part of something more.
The prevalence of patients who report with dry eye symptoms and/or present with clinical signs dictates a comprehensive whole-istic strategy of assessment and treatment. Advances in dry eye treatmentsincluding environmental engineering, awareness and training of proper blink quality and quantity, ocular lubricants, punctal plugs, therapeutic pharmaceutical agents, nutraceuticals, nutritional guidance, lid hygiene and advocacy with other health-care providerscan help improve our evaluation and management of dry eye. The debilitating nature of ocular surface disease and the degree of suffering it causes in a significant number of patients presents a demand and opportunity for creating an evaluation procedure that patients would appreciate and understand. Offer your patients this valuable evidence-based service to treat their dry eye problems as comprehensively as possibleby looking at the whole picture.
Dr. Legerton is an author and lecturer who specializes in the field of dry eye. He also holds 12 patents in the field of cornea and contact lenses. Dr. Schachet is in private practice in
1. Brewitt H, Sistani F. Dry Eye Disease: The Scale of the Problem. Surv. Ophthal 2001;45:199-201.
2. Nelson MB, Ousler GW,Nally LA, Krenzer K Alternative references values for tear break up time (TBUT) in normal and dry eye populations. Cornea 2000;19:S72.
3. Wilcox KA, Ousler GW 3rd, Schindelar MR. Effects of reflex tearing on tear film break up time (TFBUT) and tear film break-up patterns (TFBUP) in a population of Ashkenazi Jewish patients. ARVO Abstract No. 283, 2006.
4. Eye Disorders Section, Corneal Disorders, Keratoconjunctivitis Sicca. Merck Manual Online Medical Library. http://www.merck.com/mmhe/sec20/ch230/ch230d. html?qt=Keratoconjunctivitis%20Sicca&alt=sh.
5. Lane BC, Hart DE. The effects on the tear film of excessive Protein, dietary fats, alcohol, medications and depressed potassium. Report to American Public Health Assn annual meeting, 1986.
6. Nelson DW. ODs recommend omega-3, omega-6 supplements for managing dry eye. Primary Care Optometry News, November 2006.
7. Ousler GW, Lemp MA, Schindelar MR, Abelson MB. Tear film breau-up patterns (TFBUP)A method of measuring tear film stability. Poster presentation, The Tear Film and Ocular Surface Society (TFOS) meeting, 2004.
8. Guillon M, Maissa C. Bulbar conjunctival staining with contact lens wearers and non-lens wearers and its association with symptomatology. Cont. Lens Anterior Eye, 2005 June;28(2):67-73.
9. Kallarackai GU, Ansari EA, Amos N, Martin JC, Lane C, Camilleri JP. A comparative study to assess the clinical use of fluorescein meniscus time with tear break-up-time and Schirmirs test in the diagnosis of dry eyes. Eye 2002 September;16(5):594-600.
The addition of a nutraceutical to a patients diet will decrease or even
eliminate his or her dry eye.
Tear break-up time (above) and tear break-up
pattern (below) should be used and studied along with a red-thread and tear meniscus measure.
Fluorescein staining (left) and the NEI staining grid (right). Flourescein proves more useful for corneal staining, while lissamine green dye is more effective in conjunctival staining, but both will demonstrate the quality of the tear meniscus.
Blink quality and quantity may be partially to blame for your patients dry eye. Measure patients blink rate while at a computer terminal, and then discuss methods of increasing blink rate during concentrated visual tasks.
Dry eye treatment typically involves the insertion of punctal plugs, which block the tear ducts and prevent drainage.
