 A demyelinating disease is any condition that results in damage to the myelin sheath that surrounds nerve fibers in the brain and spinal cord. When the myelin sheath is damaged, nerve impulses slow or even stop, causing neurological problems.
A demyelinating disease is any condition that results in damage to the myelin sheath that surrounds nerve fibers in the brain and spinal cord. When the myelin sheath is damaged, nerve impulses slow or even stop, causing neurological problems.
Demyelinating diseases may result in vision or hearing loss, headache, seizures, muscle spasms and weakness, loss of coordination, paralysis and loss of sensation.
In the first part of this two-part column, we present an overview of demyelinating disease, with a focus on multiple sclerosis (MS)—the most common demyelinating disorder.
Myelin Basics
Myelin is a collection of lipid fats and proteins that covers the long extensions of axons. It considerably increases the speed that the action potentials move down the axons. At rest (resting potential), the neuron and the surrounding space act as a “capacitor” storing current, which is released during the action potential.1
Myelin is in both the central nervous system (CNS) and the peripheral nervous system (PNS). In the PNS, Schwann cells produce and maintain the myelin; whereas glial cells called oligodendrocytes produce and maintain the myelin in the CNS.2,3
Disorders that affect myelin interrupt nerve transmission. Patient symptoms may reflect deficits in any part of the nervous system. The most commonly affected areas in the CNS are the brain, spinal cord and optic nerves.3,4
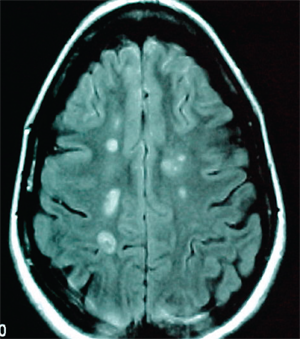
Notice the multiple ring and ovoid lesions in the periventricular and deep white matter in this patient with MS.
In primary demyelinating disorders, the cause is unknown, but an autoimmune mechanism is suspected because the disorder sometimes follows a viral infection or viral vaccination. Demyelination may also occur secondary to an infectious, ischemic, metabolic or hereditary disorder.4
MS is a chronic, recurrent disease characterized by disseminated patches of demyelination in the brain and spinal cord. But, there are also a number of other primary demyelinating disorders of the CNS (see “Non-MS Primary Demyelinating Disease of the CNS,” below).4,5
A Demyelinating Myelopathy
MS affects approximately 350,000 Americans and 2.5 million people worldwide. The prevalence of MS in the United States ranges from 6 to 177 per 100,000.1 In Western societies, MS is second only to trauma as the leading cause of neurologic disability beginning in early to middle adulthood.
The number of cases of MS appears to have steadily risen over the past century, and this increase has occurred primarily in women.1 The disease is three times more common in women than in men, with onset occurring between ages 20 and 40.1,2 Approximately 10% of cases begin before age 18; however, the disease is relatively uncommon in children under 10. Geographically, the prevalence rates of MS increase at higher latitudes.
Inflammation, demyelination and gliosis occur in patients with MS. The course can be relapsing-remitting or progressive. Symptomatic episodes consistent with MS are typically “separated in time and space”—that is, they occur months or years apart and affect different anatomical locations. As an example, a patient may present with paresthesias of the hand that resolve, followed a few months later by optic neuritis. MS is a clinical diagnosis supported by laboratory studies and neuroimaging findings.4,5
What Causes MS?
A proposed explanation for the latitude effect on MS is the possible protective power of sun exposure. Ultraviolet radiation from the sun is an important source of vitamin D, and low levels of vitamin D are common at high latitudes, particularly in winter months. Prospective studies have shown that vitamin D deficiency is associated with increased MS risk, which could be explained by the immunoregulatory effects of vitamin D.1,3
MS also correlates with high socioeconomic status, which may reflect better sanitation and thus delayed initial exposure to infectious agents. Some reports implicate specific infectious agents, such as human herpes virus type 6 or Chlamydophila pneumoniae; although, in general, the available reports have been inconsistent. A number of epidemiologic and laboratory studies suggest that an Epstein-Barr infection rarely may play a role in MS. The virus may precipitate an autoimmune process that attacks myelin. At this time, however, a causal role for Eptstein-Barr virus or any specific infectious agent remains uncertain.1,3
Non-MS Primary Demyelinating Diseases of the CNS Systems
• Optic neuritis: inflammation of the optic nerve in one or both eyes
• Neuromyelitis optica (Devic’s disease): inflammation of the optic nerve and spinal cord
• Acute transverse myelitis: inflammation of the spinal cord
• Acute disseminated encephalomyelitis: inflammation of the brain and spinal cord
• Adrenoleukodystrophy and adrenomyeloneuropathy: rare, inherited metabolic disorders
Some evidence points to a genetic influence on the development of MS, with scientists having identified a number of MS susceptibility genes.1 Whites are at higher risk than Asians and people of African descent, even when residing in a similar environment. Genetic heterogeneity may also be present in MS, meaning that there are different causative genes in different individuals.1,3 The risk of developing MS is approximately 20 times greater in first-degree relatives of patients with the disease.3
Although the precise etiology of MS remains unknown, multiple factors appear to contribute. It is thought that the immune system attacks the myelin sheath or the cells that produce and maintain it. This causes inflammation and injury to the sheath––and ultimately to the nerve fibers that it surrounds––and may result in multiple areas of scarring (sclerosis).4,5
We wish all our readers the best of systemic and ocular health in 2012! Keep an eye out for our next column in March, when we’ll discuss how to classify, diagnose and manage MS.
To read more about MS, see also “The Impact of Autoimmune Disease," under the Continuing Education tab.
1. Hauser SL, Goodin DS. Multiple sclerosis and other demyelinating diseases. In: Hauser SL, Josephson SA. Harrison’s Neurology in Clinical Medicine. 2nd edition. New York: McGraw-Hill; 2010:435-50.
2. Motor deficits. In: Simon RP, Greenberg DA, Aminoff MJ. Clinical Neurology. 7th ed. New York: McGraw-Hill; 2009:152-202.
3. The M.D. Association. Selected systemic conditions with neuro-ophthalmic signs. In: American Academy of Ophthalmology. Basic and clinical science course, section 5: neuro-ophthalmology. 2006-2007: 317-68.
4. Introduction, organization, and cellular components. In: Young PA, Young PH, Tolbert DL. Basic clinical neuroscience. 2nd ed. Philadelphia: Wolters Kluwer/Lippincott Williams & Wilkins; 2008:1-14.
5. McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol. 2001Jul;50(1):121-7.
