 Q: I just had a patient who had bilateral corneal collagen cross-linking (CXL) for post-LASIK ectasia. In one eye, she developed corneal edema and a somewhat significant hypopyon immediately following her procedure. What may have caused this? Is there anything we can do to avoid it in the future?
Q: I just had a patient who had bilateral corneal collagen cross-linking (CXL) for post-LASIK ectasia. In one eye, she developed corneal edema and a somewhat significant hypopyon immediately following her procedure. What may have caused this? Is there anything we can do to avoid it in the future?
A: Your first step should be to rule out the possibility of infection. “While infection is a rare complication of CXL, there have been a few reported cases of post-CXL infection in the literature,” says Peter Hersh, M.D., director of the Cornea and Laser Eye Institute–Hersh Vision Group in Teaneck, N.J. “Most are bacterial in origin, although herpes simplex keratitis and Acanthamoeba have been reported.”
Post-CXL infection is likely a result of the decreased epithelial barrier to microbial infiltration during the healing process after CXL rather than during the procedure itself because CXL kills bacteria and fungi in addition to damaging keratocytes.1 In some cases, a bandage contact lens that is used postoperatively may contribute, Dr. Hersh says.
A number of interventions may help to avoid infections after CXL. First, you should perform a thorough preoperative examination to look for any ocular surface disease and treat any instances of dry eye or blepharitis.
Dr. Hersh recommends the use of warm compresses, lid hygiene, tear replacement therapy, topical cyclosporine drops and topical antibiotics, as necessary to address ocular surface disease preoperatively. But, he warns against treating patients with pre-existing herpetic keratitis because of the risk of precipitating recurrent infection.
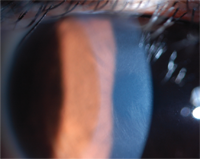
Typically, a fine corneal
haze is seen after cross-linking. Over time, this dust-like haze evolves
into a demarcation line, and subsequently resolves.
Photo: Peter Hersh, M.D.
In the early postoperative period with epithelial removal, the patient should be followed carefully until complete re-epithelialization. Typically, prophylactic antibiotics (usually a broad-spectrum fluoroquinolone) are used until the epithelium has healed completely.
“To help avoid infection, the contact lens should be removed as soon as any epithelial defect from the CXL procedure is healed,” Dr. Hersh says. “If any infiltrate, edema or hypoyon is noted, cultures should be taken as indicated and early treatment with broad-spectrum antibiotics instituted.”
Outside the setting of microbial infection, severe inflammation with hypopyon and corneal edema would be quite rare after CXL, Dr. Hersh says. Typically, a fine corneal haze is seen after cross-linking. Over time, this dust-like haze evolves into a demarcation line, and subsequently resolves.2 In rare cases, a focal, deep, scar-like haze has been described. Risk factors for such a focal scar remain unclear, but may include pre-existing corneal opacities.
Corneal edema itself is a risk of CXL. “If the cornea is too thin, the interaction of riboflavin and the ultraviolet light potentially may damage the corneal endothelium leading to corneal swelling,” Dr. Hersh says. “Treatment of eyes with appropriate corneal thickness, intraoperative stromal swelling and proper riboflavin diffusion timing should help avoid such complications.”
1. Koller T, Mrochen M, Seiler T. Complication and failure rates after corneal crosslinking. J Cataract Refract Surg. 2009 Aug; 35(8):1358-62.
2. Greenstein SA, Fry KL, Bhatt J, Hersh PS. Natural history of corneal haze after collagen crosslinking for keratoconus and corneal ectasia: Scheimpflug and biomicroscopic analysis. J Cat Refract Surg. 2010 Dec;35(12):2105-14.
