 Phototherapeutic keratectomy (PTK) uses a broad-beam excimer laser to treat corneal pathology. PTK is not new, but surgeons are developing new treatment capabilities for this technology. Here are some of them.
Phototherapeutic keratectomy (PTK) uses a broad-beam excimer laser to treat corneal pathology. PTK is not new, but surgeons are developing new treatment capabilities for this technology. Here are some of them.
When to Use It
PTK has best been used in treating these corneal disorders:
- Corneal opacities. Scars from trauma, herpes simplex or zoster, band keratopathy, Schnyder’s crystalline dystrophy and other dystrophies such as granular, lattice, macular, etc., all benefit from PTK. In one study, patients with crystalline dystrophy improved from average visual acuity of 20/175 prior to PTK to 20/40 afterward.1
- Corneal irregularity. Pterygium and pterygium surgery, Salzmann’s nodular degeneration and anterior membrane dystrophy all can cause irregular corneal surfaces. One study of PTK shows that improving the integrity of the ocular surface not only achieved normal topography results, but also improved tear film stability, ocular sensitivity, tear break-up time, and mucin production and adherence.2
- Recurrent erosion. PTK treats recalcitrant recurrent erosion well without significantly changing refractive error. This includes recurrent erosion secondary to trauma, epithelial basement membrane dystrophy; lattice, macular, Avellino or granular dystrophy; or even bullous keratopathy.3,4
A study in Singapore treated 35 eyes with PTK for recurrent erosion (16 eyes had anterior membrane dystrophy).5 All patients had exhausted conventional treatments, including hyperosmotic drops and ointments, bandage lenses and even stromal puncture. At three months after PTK, 96% of the patients were symptom free. After six months, 86% remained so.
A condition such as granular dystrophy may involve opacities, surface irregularities and recurrent erosion. PTK can treat all three pathologies concurrently.
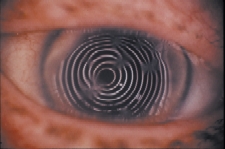 | 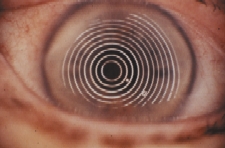 |
Salzmann’s nodular degeneration before (top) and after PTK. |
|---|
What should you bear in mind when considering a patient for PTK? The depth and location of the opacity and current refractive error are critical. In a study from Kobe, Japan, doctors treated corneal opacities less than 100 deep.6 The researchers used masking agents to prevent treatment to certain areas of the cornea and were able to significantly decrease hyperopic shift.
The location of the pathology determines the induced refractive change. Peripheral pathologies such as Salzmann’s degeneration can manifest a hyperopic shift after PTK. A patient with a refractive error of +3.00D might be a less suitable candidate than one who is -2.00D. Likewise, a central opacity will have a myopic shift post-op. Generally, the deeper the pathology, the greater the amount of tissue removed, and the greater the change in refractive error. One rare occurrence following PTK is the development of stromal haze.
But overall, PTK is safe and effective, and promises new options for treating patients with corneal opacities, surface irregularities and recurrent erosions.
< LEFTMARGIN="30" RIGHTMARGIN="30">
1. Paparo LG, Rapuano CJ, Raber IM, et al. Phototherapeutic keratectomy for Schnyder’s crystalline corneal dystrophy. Cornea 2000 May;19(3):343-7.
2. Dogru M, Katakami C, Miyashita M, et a.. Ocular surface changes after excimer laser phototherapeutic keratectomy. Ophthalmology 2000 Jun;107(6):1144-52.
3. Lin PY, Wu CC, Lee SM. Combined phototherapeutic keratectomy and therapeutic contact lens for recurrent erosions in bullous keratopathy. Br J Ophthalmol 2001 Aug; 85(8):908-11.
4. Maini R, Sullivan L, Snibson GR, et al. A comparison of different depth ablations in the treatment of painful bullous keratopathy with phototherapeutic keratectomy. Br J Ophthalmol 2001 Aug;85(8):912-5.
5. Ho CL, Tan DT, Chan WK. Excimer laser phototherapeutic keratectomy for recurrent corneal erosions. Ann Acad Med Singapore 1999 Nov;28(6):787-90.
6. Dogru M, Katakami C, Yamanaka A. Refractive changes after excimer laser phototherapeutic keratectomy. J Cataract Refract Surg 2001 May;27(5):686-92.
