Pachymetry is the standard of care. You cant practice optometry now without measuring corneal thickness, says optometrist Louis J. Phillips.
Dr. Phillips, a private practitioner as well as owner and director of Sightline Laser Eye Center in Pittsburgh, echoes the same sentiment expressed by the other specialists interviewed for this article: A pachymeter is a now required for glaucoma risk evaluation and management.
This happened, of course, in light of the results from the Ocular Hypertension Treatment Study, among many other studies, which have found that the thickness of the cornea affects the measurement of intraocular pressure.1,2
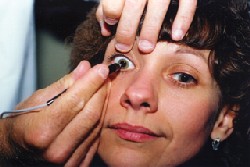
Pachymetry is now standard of care for optometryand not only for glaucoma care. Courtesy: Jeffrey Augustine, O.D.
Not every patient needs to have a central corneal thickness measurement, he says. But for many people who come through optometric practices, you will eventually need this information to accurately assess risk for the development of glaucoma. Yet, he adds, it may be prudent to take a baseline reading not only on glaucoma suspects, but also on other patients.
To that end, you can put your new pachymeter to use in several ways. Very likely, youll be using it when you refer patients for refractive surgery. But you may also use your pachymeter to monitor ortho-K patients, extended wear and problem contact lens patients, and even dry eye patients. Heres how.
Corneal Reshaping Pachymetry Gets a CPT Code
You can call it orthokeratology. Or, if you use the Paragon lenses, you can call it Corneal Refractive Therapy. Optometrist Bill Berkea contact lens specialist whos been fitting patients with reverse geometry lenses for years at his Santa Ana, Calif., practicerefers to the method of treatment as corneal reshaping.
Dr. Berke has also been using ultrasound pachymetry to monitor changes in the epithelial thickness of patients undergoing corneal reshaping. His observations may turn the current understanding of corneal reshaping on its ear.
Previous research suggests that corneal reshaping leads to a flattened central cornea and a thickened midperiphery. In 1998, researchers at the School of Optometry of the University of New South Wales studied six subjects (11 eyes) undergoing orthokeratology. Using an optical pachymeter, the researchers observed central epithelial thinning, as well as midperipheral corneal thickening.3

In a LASIK procedure, the surgeon uses the pachymeter intraoperatively to calculate a more accurate flap thickness.
Later studies using optical pachymeters also observed central corneal thinning.4
But thats not what Dr. Berke has found. He does agree with the conclusion that reverse geometry lenses lead to a thicker midperipheral cornea. But he disagrees that this effect is linked to migration of cells and compression of the central corneal epithelium.
When I got an ultrasound pachymeter sensitive enough to measure the epithelium separately from the total thickness of the cornea, I was finding that the center epithelium was not thinning at all, Dr. Berke says. I was getting the same measurements, within normal standard deviation, before I applied the corneal reshaping contact lens and then after I got complete results.
The cells of the epithelium are composed mostly of water, he says, which make them too dense to be compressed. However, the cells can expandor hypertrophyand that explains how the cells at the midperiphery bulge into the negative space of the reverse geometry lens, Dr. Berke says.
While hes made this observation on numerous patients, Dr. Berke plans a formal research study that will start in the spring. He knows of a similar study, currently under way, that is already yielding the same findings.
The lynchpin of his observations, he says, is his use of a high frequency (50MHz) ultrasound pachymeter that is precise enough to measure the thin (about 50m) corneal epithelium.
LASIK Comanagement
Not only has pachymetry become standard of care for glaucoma, its long been vital for refractive surgery comanagement.
Optometrists without pachymeters need to refer patients with higher prescriptions to the laser center simply to get the patients corneal thickness checked as a prerequisite before surgery, says Jeffrey Augustine, O.D., clinical director at Clear Choice Laser Eye Center, Brecksville, Ohio. This helps prevent patient and doctor disappointment on the day of surgery, should the patient have corneas that are too thin for refractive surgery.
It would be easier on the patientespecially a high myope or keratoconus suspectif the comanaging doctor discerned whether the patient is a candidate for refractive surgery prior to the day of surgery, Dr. Augustine says. This means measuring the corneal thickness before sending the patient to the surgery center.
As of January 2004, pachymetry received its own official Current Procedural Technology (CPT) code: 76514. This replaces 2003s temporary code for pachymetry, 0025T.
Medicares reimbursement of this diagnostic procedure will yield an average of $12.34 in 2004. Generally, for ocular hypertensives and glaucoma patients, this will be reimbursed on a once-in-a-lifetime basis, explains optometrist Charles Brownlow, executive vice president of the Wisconsin Optometric Association and a consultant on billing and coding.
Dr. Brownlow performed a survey last year (for Sonogage) on state Medicare policies for pachymetry, before this years national policy was enacted. He found that Medicare reimbursements in various states ranged from as low as $20 to as high as $115. He expects that doctors are setting their fees for pachymetry along a similarly wide spectrum.
At a minimum to participate in comanagement, optometrists should have a corneal topographer and a pachymeter, and that way they can discuss corneal thickness or know if theres a red flag before the patient is ever referred to a laser center, says Wally Ryne, O.D., owner of Clear View Laser Vision Center, near Ft. Worth, Texas.
Following a growing trend in refractive surgery, surgeons at Dr. Rynes center now use an ultrasound pachymeter to take an intraoperative reading. Its called subtraction pachymetry, and it gives a more accurate reading of the flap thickness.
After creating the flap, the surgeon places the pachymeter probe on the corneal bed. Subtract the thickness of the corneal bed from the total corneal thickness, and you have the flap thicknessan essential datum for patients who may require enhancement or retreatment, Dr. Ryne explains.
Pachymetry has become a standard part of the LASIK procedure, he says, and a necessary instrument in comanaging doctors offices. With roughly 4,000 LASIK procedures being performed everyday in the U.S., optometrists are going to see more and more of these patients in their clinics, Dr. Ryne says.
Pachymetry Aids Both Glaucoma Diagnosis and Management
Corneal Pathology
Researchers continue to connect the dots between corneal thickness and glaucoma development. Last month, researchers at Duke University Eye Center published a study that confirmed central corneal thickness, measured at the initial exam, can help determine the severity of the disease.9 They found that primary open-angle glaucoma patients who have thinner central corneal thickness tend to have more severe glaucomatous damage.
Theres a relationship between corneal thickness and intraocular pressure, thats for sure, Dr. Phillips says. But, he adds, clinicians shouldnt rely too heavily yet on the certainty of this relationship. He says that the underlying nature of the relationship between corneal thickness and IOP is still unclear. "We dont know, as the cornea gets thicker, whether its a linear relationship or a nonlinear relationship," he says. And, at this point, central corneal thickness (CCT) conversion charts that translate measured IOP into adjusted IOP provide only guesstimates, at best.
Still, knowing CCT has helped to sharpen the diagnosis of at-risk glaucoma patients, Dr. Phillips says. But bear in mind that it also helps in managing those patients. For example, a patient with thin corneas and high IOPs should indeed tip the doctors hand toward starting the patient on medication. But the low CCT should also influence management, so the doctor should aim target pressures much lower than for a similar patient with thicker corneas.
As an addition to, or confirmation of, other methods, pachymetry can signal corneal pathologies such as keratoconus, Fuchs dystrophy, pellucid marginal degeneration and Terriens degeneration, says Dr. Berke. You can use the pachymeter for diagnosis (to identify certain thinned spots on the cornea), and for monitoring (to make a record of a degenerative process).
In the worst cases, for example, excessive thinning could dictate the need for a corneal transplant.
Extended Wear
Extended wear contact lens patients who suddenly present with blurred vision or reduced acuity may have developed corneal edema. If you had taken baseline pachymetry readings, Dr. Berke says, you could now take another reading to confirm corneal edema.
Also, some patients may experience corneal changes, such as inferior steepening or warpage of the cornea. So it may be helpful to take a baseline corneal thickness on any specialty contact lens patient in case changes occur, Dr. Berke suggests.
Pay particular attention to extended wear patients, as overnight extended wear contact lenses have shown to slightly decrease central corneal thickness over time.5,6
Dry Eye
Interestingly, dry eyes have also been shown to affect central corneal thickness. One study from the Bascom Palmer Eye Institute showed about 6% reduction in central corneal thickness in dry eyes compared with normal eyes.7 So, in certain cases, pachymetry could be helpful as an additionaland objectivemeasure to record improvement with a dry eye treatment regimen.
In addition, a recent study found that corneal drying for one minutes duration decreased corneal thickness by 3%, which in turn may affect measured IOP.8 Applanation tonometry may underestimate IOP if the patient is restrained from blinking during measurement, the authors write. The take-home message: Let your patients blink between tonometry readings.
Now that you know what you can use your pachymeter for, heres a tip on how to use it (for ultrasound pachymeters): Position the probe on the center cornea and hold it perpendicular to the eye. Dont press against the corneal tissue, Dr. Berke says. Just bring the tip to the cornea light enough to make contact.
Take several readings, he says, but dont average them since one outlier could throw off the number. Youll usually want to use the lowest of the readings, which indicates when you held the probe at its most perpendicular. Its a simple procedure, and one that a technician can learn easily.
1. Gordon MO, Beiser JA, Brandt JD, et al. The Ocular Hypertension Treatment Study: baseline factors that predict the onset of primary open-angle glaucoma. Arch Ophthalmol 2002 Jun; 120(6): 714-20.
2. Phillips LJ, Cakanac CJ, Eger MW, Lilly ME. Central corneal thickness and measured IOP: a clinical study. Optometry 2003 Apr; 74(4): 218-25.
3. Swarbrick HA, Wong G, O"Leary DJ. Corneal response to orthokeratology. Optom Vis Sci 1998 Nov; 75(11): 791-9.
4. Soni PS, Nguyen TT, Bonanno JA. Overnight orthokeratology: visual and corneal changes. Eye Contact Lens 2003 Jul; 29(3): 137-45.
5. Gurdal C, Aydin S, Kirimlioglu H, et al. Effects of extended-wear soft contact lenses on the ocular surface and central corneal thickness. Ophthalmologica. 2003 Sep-Oct; 217(5): 329-36.
6. Ren DH, Yamamoto K, Ladage PM, et al. Adaptive effects of 30-night wear of hyper-O(2) transmissible contact lenses on bacterial binding and corneal epithelium: a 1-year clinical trial. Ophthalmology 2002 Jan; 109(1): 27-39; discussion 39-40.
7. Liu Z, Pflugfelder SC. Corneal thickness is reduced in dry eye. Cornea 1999 Jul; 18(4): 403-7.
8. Dayanir V, Sakarya R, Ozcura F, et al. Effect of corneal drying on central corneal thickness. J Glaucoma 2004 Feb; 13(1): 6-8.
9. Herndon LW, Weizer JS, Stinnett SS. Central corneal thickness as a risk factor for advanced glaucoma damage. Arch Ophthalmol 2004 Jan; 122(1): 17-21.
