 |  |
Patients with recurrent corneal erosions (RCE) typically experience sudden onset of eye pain on first awakening. Associated symptoms include redness, photophobia, blurred vision and tearing. Pain may last from minutes to several hours, and, in the most severe cases with persistent epithelial defects, patients can experience pain for several days.
Many patients with RCE have a history of corneal trauma, corneal dystrophies and degenerations or previous surgery that may predispose them to the condition. Other times, the RCE can occur spontaneously due to preexisting dystrophies or diabetes. In all cases, RCE is characterized by a disturbance at the corneal epithelial basement membrane, resulting in defective adhesions and recurrent breakdowns of the epithelium.
By asking the right questions and performing a thorough examination, we can successfully diagnose our patients and treat them accordingly the majority of the time. Ocular signs found on slit lamp include punctate epitheliopathy, corneal abrasions, loose and/or irregular epithelium and cystic and map-like changes associated with EBMD.1
Although we can identify the signs and symptoms, patients may have corneal erosions in the absence of visible corneal findings. The cornea sweep test is a new and effective technique to help diagnose corneal erosions. Using this test could lead to a paradigm shift in the way clinicians approach RCEs and patients with a persistent ocular pain syndrome. A handheld instrument with a straight handle and rounded tip with smooth and tapered edges sweeps the entire corneal surface to identify the areas of loose epithelium.2 Topical proparacaine eye drops and fluorescein dye are instilled and gentle pressure is applied to the corneal surface tangentially with the instrument.2
The cornea sweep test was necessary on 49 of 58 eyes in one study to help confirm a corneal erosion diagnosis. In 34 eyes that had an occult corneal erosion, they were initially defined with a normal-appearing cornea on slit lamp examination but found to have loose corneal epithelium with the test.2
 |
|
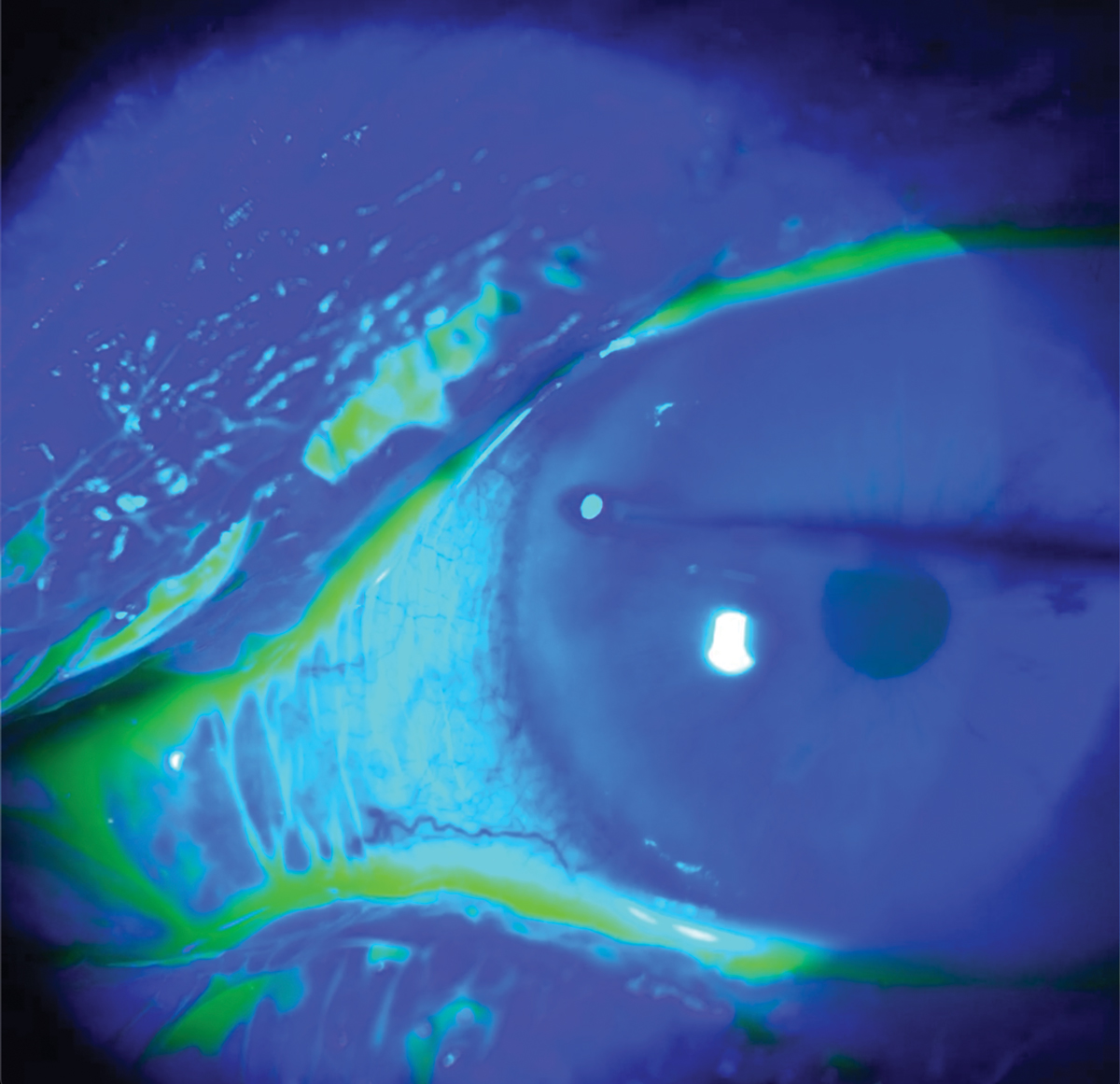
The cornea sweep test can help identify this acute and chronic condition. Photo: Brian Kim, MD. Click image to enlarge. |
Choice of Therapy
No matter the cause, various medical, conservative and surgical treatments are available. Medical options include lubrication using preservative-free artificial tears, pressure patching and cycloplegia to help promote surface healing, topical antibiotics to prevent bacterial infection with existing epithelial topical corticosteroids and oral doxycycline.1,3-5 Bandage contact lenses, punctal occlusion, autologous serum and amniotic membranes are additional measures.1
For patients who suffer from repeated episodes of RCE, our threshold for referral for corneal surgeries is low, and we frequently make one after the first repeat, depending on initial appearance. These procedures are reserved after failed medical therapy.
Anterior stromal puncture (ASP), phototherapeutic keratectomy (PTK), Nd:YAG laser or epithelial debridement with diamond burr polishing can help address the underlying cause of poor basement membrane adhesion. Surgical success rates for RCE vary from ASP at 80%. PTK varies from 60% to 100% depending on the study, and epithelial debridement with diamond burr polishing decreases the recurrence rate to 6% when compared with debridement alone (18%).1,3,6
Proper identification is key to address RCE. Many symptoms and signs may overlap between it and a variety of ocular surface diseases. Using novel diagnostic techniques, we can help identify this acute and chronic condition to treat and minimize patient suffering.
1. Miller DD, Hasan SA, Simmons NL, Stewart MW. Recurrent corneal erosion: a comprehensive review. Clin Ophthalmol. 2019;13:325-35. 2. Kim ME, Kim DB. Implementation of the corneal sweep test in the diagnosis of recurrent corneal erosion: a two-year retrospective study. Cornea. 2022;41(10):1248-54. 3. Lin SR, Aldave AJ, Chodosh J. Recurrent corneal erosion syndrome. Br J Ophthalmol. 2019;103:1204-8. 4. Sobrin L, Liu Z, Monroy DC, et al. Regulation of MMP-9 activity in human tear fluid and corneal epithelial culture supernatant. Invest Ophthalmol Vis Sci. 2000;4:1-7. 5. Dursun D, Kim M, Solomon A, Pflugfelder S. Treatment of recalcitrant recurrent corneal erosions with inhibitors of matrix metalloproteinase-9, doxycycline and corticosteroids. Am J Ophthalmol. 2001;132:8-13. 6. Wong VW, Chi SC, Lam DS. Diamond burr polishing for recurrent corneal erosions: results from a prospective randomized controlled trial. Cornea. 2009;28(2):152-6. |
