Myopia affects approximately 70 million Americans.1 It is associated with potentially sight-threatening side effects, and it costs the United States up to $4.6 billion every year.2-4
Finding a treatment that slows the progression of myopia or even prevents its onset will have a dramatic affect on individual patients lives and society in general. While researchers have compiled considerable information about myopia over the past several years, controversy regarding its primary cause still exists.
We can broadly categorize potential causes of myopia and myopia progression into two theories: genetic or environmental. Through animal and human trials, researchers have gathered evidence for and against each theory. So far, however, no single study has proven either theory correct. Most likely, no study will provide definitive evidence that one theory alone can fully explain how people become myopic.
|
|
|
A young, myopic patient participates in a myopia control clinical trial. |

Genetics vs. Environment
Evidence of a genetic etiology includes the high heritability (approximately 0.90) of myopia.5-7 Monozygotic twins also have higher heritability than dizygotic twins, and the refractive error of twins is highly correlated.5-10
Furthermore, research has shown that emmetropic children who have two myopic parents have longer eyes than emmetropic children who have one myopic parent and that children who have one myopic parent have longer eyes than children who have no myopic parents.11 Researchers have also found that parental history of myopia at school entry has excellent sensitivity (0.90) for predicting the future onset of myopia and is associated with higher rates of myopia progression in children.12,13
These findings all indicate a strong propensity for myopia to be passed from one generation to the next. However, no single gene has been mapped for high myopia or moderate myopia.14-20 Perhaps, this is because multiple gene loci are involved in myopia development and progression.
Some of these factors suggest that the tendency for myopia is passed from generation to generation. However, it is difficult to separate the effects of genes from similar environments because siblings are typically raised in similar environments in which similar factors, such as near visual activities, may affect myopia progression.
Evidence for an environmental cause of myopia includes the possibility of an epidemic of myopia in specific populations.21-23 Francis Young, Ph.D., was among the first to report this phenomenon.24 He and his colleagues reported a refractive error correlation equivalent to zero between parents and children in an Eskimo population, while siblings had a refractive error correlation of approximately 0.5.23 The Eskimo parents and grandparents had nearly no myopia, yet approximately three out of five children were nearsighted.
The authors concluded that this was due to the recent onset of formalized education, which engaged children in more reading and led to the development of myopia. This sudden increase in the prevalence of myopia in Eskimos and similar trends in Asia are difficult to explain by genetics alone because it has been reported to occur within one or two generations.25-28
Confounding Factors
It is unclear whether there truly is an epidemic of myopia or whether confounding factors suggest a sudden rise in the prevalence of myopia. For example, changes in the ethnic profile of a particular area may explain changes in the prevalence of myopia. One study found that the prevalence of myopia in a northern California community doubled over 30 yearsa finding that researchers attribute to an influx of Asian-American children in the area.29
Similarly, changes in the age distribution of a particular area could explain a sudden increase in the prevalence of myopia. Cross-sectional studies show that the prevalence of myopia is approximately two times greater for people in their 40s than people in their 70s.30, 31 If a community was suddenly infused with a younger population, it may appear that the mean refractive error of the community could change dramatically. In reality, though, the younger age distribution of the population could explain the apparent shift in myopia prevalence. A difference in age could explain the difference in the prevalence of myopia between generations of Eskimos in Dr. Youngs cross-sectional study.23
The possibility of an epidemic of myopia is stirring. Even so, we must not draw unwarranted conclusions without more rigorous examinations of potential causes of sudden reported increases in the prevalence of myopia.
Current Therapies
Many current therapies are geared toward alleviating potential environmental effects on myopia progression. One current theory is that accommodative lag experienced by young children leads to myopic eye growth due to light focusing posteriorly on the retina. Indeed, several animal studies show that hyperopic blur detected within the eye results in faster axial elongation and myopic development.32-34
Controversy exists regarding the onset of accommodative error in young, incipient myopes. Jane Gwiazda, Ph.D., and colleagues found that increased accommodative lag occurs prior to the onset of myopia, while Donald Mutti, O.D., and colleagues contend that increased accommodative lag occurs before myopia onset.35,36 If the latter is true, then accommodative lag does not explain the onset of myopia but is a result of myopia onset.
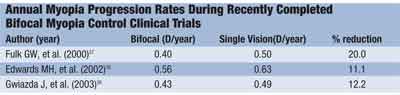
Bifocal spectacles. These decrease the accommodative demand for young children and, as a result, the accommodative error they experience. However, three recently completed randomized clinical trials show little to no treatment effect by bifocal spectacle lenses, indicating that accommodative lag plays a minor, if any, role in increased myopic progression in children.37-39 (See Annual Myopia Progression Rates During Recently Completed Bifocal Myopia Control Clinical Trials, above.)
An auxiliary study is examining the potential treatment effect of bifocal spectacles for a subset of children who have low myopia, high accommodative lag and nearpoint esophoria.40 Results from this study will help elucidate the role of accommodative error in myopia development.
Undercorrection of myopia is similar to wearing a bifocal and should lead to decreased accommodative effort and improved near vision. This would result in decreased myopia progression. However, a randomized trial found that undercorrection of myopia actually increased the progression.41 Treatment of accommodative error, the most commonly hypothesized environmental cause of myopia development, has not yet proven to be fruitful, but other environmental theories have been proposed.
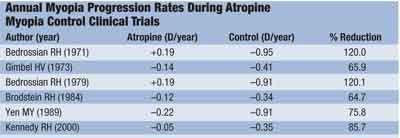
In other studies, researchers evaluated specific receptors in the retina for myopia control using pirenzepinea selective muscarinic antagonist reported to minimally affect accommodation. They found that pirenzepine reduced axial eye growth in lens-induced refractive errors of animals.55-57 Randomized clinical trials in humans have proven that application of the ophthalmic gel slows the progression of myopia in children.58,59 In both studies, myopia progression was reduced to nearly half that of the control subjects after one year. About one in 10 subjects withdrew from the study due to side effects of the drug. Still, all subjects fully recovered from any ill effects they exhibited. The FDA has not approved this treatment, so it is not available in the United States.
Elevated intraocular pressure is another factor that researchers have investigated as a possible contributor to myopia. One hypothesis: Higher IOP, perhaps in combination with a weaker scleral shell, leads to increased globe expansion and greater axial elongation.60-62 A study of chicks showed that timolol maleate lowers IOP but does not slow the growth of the eyes. One study in humans showed that IOP-lowering agents are unsuccessful at slowing the progression of nearsightedness in children.63
Animal models of blur-driven myopia development have shown that brief periods of unrestricted vision can greatly decrease or eliminate myopic eye growth.64,65 This finding indicates that a blur-driven cause of myopia development must be relatively constant and would argue against accommodative error as a cause for myopia development. Higher-order aberrations lead to sustained minute levels of blur on the retina and are currently being examined as a potential initiator for myopia development.66,67

An animal model of myopia indicates that the midperipheral portion of the retina may play a stronger role in eye growth regulation than the central retina, so patients may experience clear vision while benefiting from slowed eye growth as images focus in front of the peripheral retina.70 Determining potential causes of myopia, such as higher order aberrations leading to myopic eye growth (discussed previously), may lead to future treatments for myopia progression.
Neither genetic nor environmental factors alone explain the onset or progression of myopia. However, environmental and genetic causes may play integrated roles in the development of myopia.
For example, a subset of children may carry specific genes that make them susceptible to the effects of accommodative error. These children will become myopic if they exhibit an accommodative lag to near stimuli, while children who are not genetically susceptible will remain emmetropic, even when they exhibit a large accommodative lag while reading. To determine whether this may be true, scientists have searched for a gene-environment interaction, but no such interaction has been reported to date.
Although two distinct camps exist regarding the cause of myopia development and progression, it is likely that a combination of the two general causes will partially explain how people become nearsighted.
Dr. Walline is an Assistant Professor at the Ohio State University (OSU) College of Optometry. He served as chairman of the Contact Lens and Myopia Progression (CLAMP) Studya randomized clinical trial to examine the effects of gas permeable contact lens wear on myopia progression in children. He currently is the principal investigator of the Adolescent and Child Health Initiative to Encourage Vision Empowerment (ACHIEVE) Studya randomized clinical trial to investigate the effects of contact lens wear on nearsighted childrens self-perception, and is conducting the Corneal Reshaping and Yearly Observation of Nearsightedness (CRAYON) Study to examine the effects of corneal reshaping contact lenses on myopia progression in children.
1. Sperduto RD, Seigel D, Roberts J, Rowland M. Prevalence of myopia in the United States. Arch Ophthalmol 1983 Mar; 101(3):405-7.
2. Saw SM, Gazzard G, Shih-Yen EC, Chua WH. Myopia and associated pathological complications. Ophthalmic Physiol Opt 2005 Sep;25(5):381-91.
3. Risk factors for idiopathic rhegmatogenous retinal
detachment. The Eye Disease Case-Control Study Group. Am J Epidemiol 1993 Apr 1;137(7):749-57.
4. Javitt JC, Chiang YP. The socioeconomic aspects of laser refractive surgery. Arch Ophthalmol 1994 Dec;112(12):
1526-30.
5. Teikari JM, Kaprio J, Koskenvuo MK, Vannas A. Heritability estimate for refractive errorsa population-based sample of adult twins. Genet Epidemiol 1988;5(3):171-81.
6. Lyhne N, Sjolie AK, Kyvik KO, Green A. The importance of genes and environment for ocular refraction and its determiners: a population based study among 20-45 year old twins. Br J Ophthalmol 2001 Dec;85(12):1470-6.
7. Hammond CJ, Snieder H, Gilbert CE, Spector TD. Genes and environment in refractive error: the twin eye study. Invest Ophthalmol Vis Sci 2001 May;42(6):1232-6. 2001 May; 42(6):1232-6.
8. Teikari JM, ODonnell J, Kaprio J, Koskenvuo M. Impact of heredity in myopia. Hum Hered 1991;41(3):151-6.
9. Saw SM, Chua WH, Wu HM, et al. Myopia: gene-environment interaction. Ann Acad Med Singapore 2000 May;29(3):290-7.
10. Teikari JM, Kaprio J, Koskenvuo M, ODonnell J. Heritability of defects of far vision in young adultsa twin study. Scand J Soc Med 1992 Jun;20(2):73-8.
11. Zadnik K, Satariano WA, Mutti DO, et al. The effect of parental history of myopia on childrens eye size. JAMA 1994 May 4;271(17):1323-7.
12. Mutti DO, Zadnik K. The utility of three predictors of childhood myopia: a Bayesian analysis. Vision Res 1995 May;35(9):1345-52.
13. Saw SM, Nieto FJ, Katz J, et al. Familial clustering and myopia progression in Singapore school children. Ophthalmic Epidemiol 2001 Sep;8(4):227-36.
14. Young TL, Ronan SM, Drahozal LA, et al. Evidence that a locus for familial high myopia maps to chromosome 18p. Am J Hum Genet 1998 Jul;63(1):109-19.
15. Young TL, Atwood LD, Ronan SM, et al. Further refinement of the MYP2 locus for autosomal dominant high myopia by linkage disequilibrium analysis. Ophthalmic Genet 2001 Jun;22(2):69-75.
16. Young TL, Ronan SM, Alvear AB, et al. A second locus for familial high myopia maps to chromosome 12q. Am J Hum Genet 1998 Nov;63(5):1419-24.
17. Paluru PC, Nallasamy S, Devoto M, et al. Identification of a novel locus on 2q for autosomal dominant high-grade myopia. Invest Ophthalmol Vis Sci 2005 Jul;46(7):2300-7.
18. Paluru P, Ronan SM, Heon E, et al. New locus for autosomal dominant high myopia maps to the long arm of chromosome 17. Invest Ophthalmol Vis Sci 2003 May;44(5): 1830-6.
19. Hammond CJ, Andrew T, Mak YT, Spector TD. A susceptibility locus for myopia in the normal population is linked to the PAX6 gene region on chromosome 11: a genomewide scan of dizygotic twins. Am J Hum Genet 2004 Aug;75(2): 294-304.
20. Stambolian D, Ibay G, Reider L, et al. Genomewide linkage scan for myopia susceptibility loci among Ashkenazi Jewish families shows evidence of linkage on chromosome 22q12. Am J Hum Genet 2004 Sep;75(3):448-59.
21. Riegelman RK. Medical Student Myopia Syndrome: a recently recognized pan-epidemic. Am J Prev Med 1991 Jul-Aug;7(4):252.
22. Morgan RW, Speakman JS, Grimshaw SE. Inuit myopia: an environmentally induced epidemic? Can Med Assoc J 1975 Mar 8;112(5):575-7.
23. Young FA, Leary GA, Baldwin WR, et al. The transmission of refractive errors within eskimo families. Am J Optom Arch Am Acad Optom 1969;46:676-85.
24. Young F, Leary G, Baldwin W, et al. The transmission of refractive errors within Eskimo families. American Journal of Optometry and Archives of American Academy of Optometry 1969;47:244-9.
25. Mutti DO, Bullimore MA. Myopia: an epidemic of possibilities? Optom Vis Sci 1999 May;76(5):257-8.
26. Grosvenor T. Why is there an epidemic of myopia? Clin Exp Optom 2003 Sep;86(5):
273-5.
27. Park DJ, Congdon NG. Evidence for an epidemic of myopia. Ann Acad Med Singapore 2004 Jan;33(1):21-6.
28. Junghans BM, Crewther SG. Little evidence for an epidemic of myopia in Australian primary school children over the last 30 years. BMC Ophthalmol 2005 Feb 11;5(1):1.
29. Zadnik K. The Glenn A. Fry Award Lecture (1995). Myopia development in childhood. Optom Vis Sci 1997 Aug;74(8):603-8.
30. Wang Q, Klein BE, Klein R, Moss SE. Refractive status in the Beaver Dam Eye Study. Invest Ophthalmol Vis Sci 1994 Dec;35(13):4344-7.
31. Katz J, Tielsch JM, Sommer A. Prevalence and risk factors for refractive errors in an adult inner city population. Invest Ophthalmol Vis Sci 1997 Feb;38(2):334-40.
32. Smith EL 3rd. Spectacle lenses and emmetropization: the role of optical defocus in regulating ocular development. Optom Vis Sci 1998 Jun;75(6):388-98.
33. Norton TT, Siegwart JT Jr. Animal models of emmetropization: matching axial length to the focal plane. J Am Optom Assoc 1995 Jul;66(7):405-14.
34. Troilo D, Wallman J. The regulation of eye growth and refractive state: an experimental study of emmetropization. Vision Res 1991;31(7-8):1237-50.
35. Gwiazda J, Thorn F, Held R. Accommodation, accommodative convergence, and response AC/A ratios before and at the onset of myopia in children. Optom Vis Sci 2005 Apr;82(4):273-8.
36. Mutti DO, Mitchell GL, Hayes JR, et al. Accommodative lag before and after the onset of myopia. Invest Ophthalmol Vis Sci 2006 Mar;47(3):837-46.
37. Fulk GW, Cyert LA, Parker DE. A randomized trial of the effect of single-vision vs. bifocal lenses on myopia progression in children with esophoria. Optom Vis Sci 2000 Aug; 77(8):395-401.
38. Gwiazda J, Hyman L, Hussein M, et al. A randomized clinical trial of progressive addition lenses versus single vision lenses on the progression of myopia in children. Invest Ophthalmol Vis Sci 2003 Apr;44(4):1492-500.
39. Edwards MH, Li RW, Lam CS, et al. The Hong Kong progressive lens myopia control study: study design and main findings. Invest Ophthalmol Vis Sci 2002 Sep;43(9):2852-8.
40. Gwiazda JE, Hyman L, Norton TT, et al. Accommodation and related risk factors associated with myopia progression and their interaction with treatment in COMET children. Invest Ophthalmol Vis Sci 2004 Jul;45(7):2143-51.
41. Chung K, Mohidin N, OLeary DJ. Undercorrection of myopia enhances rather than inhibits myopia progression. Vision Res 2002 Oct;42(22):2555-9.
42. Lee JJ, Fang PC, Yang IH, et al. Prevention of myopia progression with 0.05% atropine solution. J Ocul Pharmacol Ther 2006 Feb;22(1):41-6.
43. Gimbel HV. The control of myopia with atropine. Can J Ophthalmol 1973 Oct;8(4):527-32.
44. Yen MY, Liu JH, Kao SC, Shiao CH. Comparison of the effect of atropine and cyclopentolate on myopia. Ann Ophthalmol 1989 May;21(5):180-2, 187.
45. Romano PE, Donovan JP. Management of progressive school myopia with topical atropine eyedrops and photochromic bifocal spectacles. Binocul Vis Strabismus Q 2000;15(3):257-60.
46. Kennedy RH. Progression of myopia. Trans Am Ophthalmol Soc 1995;93:755-800.
47. Pointer RW. Atropine and photochromic bifocals for 800 cases of school myopia. Binocul Vis Strabismus Q 2000;15(3):256.
48. Shih YF, Chen CH, Chou AC, et al. Effects of different concentrations of atropine on controlling myopia in myopic children. J Ocul Pharmacol Ther 1999 Feb;15(1):85-90.
49. Chou AC, Shih YF, Ho TC, Lin LL. The effectiveness of 0.5% atropine in controlling high myopia in children. J Ocul Pharmacol Ther 1997 Feb;13(1):61-7.
50. Brodstein RS, Brodstein DE, Olson RJ, et al. The treatment of myopia with atropine and bifocals. A long-term prospective study. Ophthalmology 1984 Nov;91(11):1373-9.
51. Bedrossian RH. The effect of atropine on myopia. Ophthalmology 1979 May;86(5):713-9.
52. Bedrossian RH. The effect of atropine on myopia. Ann Ophthalmol 1971 Aug;3(8):891-7.
53. Shih YF, Hsiao CK, Chen CJ, et al. An intervention trial on efficacy of atropine and multi-focal glasses in controlling myopic progression. Acta Ophthalmol Scand 2001 Jun; 79(3):233-6.
54. Troilo D, Gottlieb MD, Wallman J. Visual deprivation causes myopia in chicks with optic nerve section. Curr Eye Res 1987 Aug;6(8):993-9.
55. Cottriall CL, McBrien NA. The M1 muscarinic antagonist pirenzepine reduces myopia and eye enlargement in the tree shrew. Invest Ophthalmol Vis Sci 1996 Jun;37(7):1368-79.
56. Rickers M, Schaeffel F. Dose-dependent effects of intravitreal pirenzepine on deprivation myopia and lens-induced refractive errors in chickens. Exp Eye Res 1995 Oct;61(4): 509-16.
57. Stone RA, Lin T, Laties AM. Muscarinic antagonist effects on experimental chick myopia. Exp Eye Res 1991 Jun;52(6): 755-8.
58. Tan DT, Lam DS, Chua WH, et al. One-year multicenter, double-masked, placebo-controlled, parallel safety and efficacy study of 2% pirenzepine ophthalmic gel in children with myopia. Ophthalmology 2005 Jan;112(1):84-91.
59. Siatkowski RM, Cotter S, Miller JM, et al. Safety and efficacy of 2% pirenzepine ophthalmic gel in children with myopia: a 1-year, multicenter, double-masked, placebo-controlled parallel study. Arch Ophthalmol 2004;122:1667-74.
60. Jensen H. Myopia progression in young school children and intraocular pressure. Doc Ophthalmol 1992;82(3):
249-55.
61. Quinn GE, Berlin JA, Young TL, et al. Association of intraocular pressure and myopia in children. Ophthalmology 1995 Feb;102(2):180-5.
62. Edwards MH, Brown B. IOP in myopic children: the relationship between increases in IOP and the development of myopia. Ophthalmic Physiol Opt 1996 May;16(3):243-6.
63. Jensen H. Myopia progression in young school children. A prospective study of myopia progression and the effect of a trial with bifocal lenses and beta blocker eye drops. Acta Ophthalmol Suppl 1991;200:1-79.
64. Smith EL 3rd, Hung LF, Kee CS, Qiao Y. Effects of brief periods of unrestricted vision on the development of form-deprivation myopia in monkeys. Invest Ophthalmol Vis Sci 2002 Feb;43(2):291-9.
65. Nickla DL, Sharda V, Troilo D. Temporal integration characteristics of the axial and choroidal responses to myopic defocus induced by prior form deprivation versus positive spectacle lens wear in chickens. Optom Vis Sci 2005 Apr;82(4):318-27.
66. Charman WN. Aberrations and myopia. Ophthalmic Physiol Opt 2005 Jul;25(4):285-301.
67. Roberts B, Athappilly G, Tinio B, et al. Higher order aberrations induced by soft contact lenses in normal eyes with myopia. Eye Contact Lens 2006 May;32(3):138-42.
68. Walline JJ, Jones LA, Mutti DO, Zadnik K. A randomized trial of the effects of rigid contact lenses on myopia progression. Arch Ophthalmol 2004 Dec;122(12):1760-6.
69. Katz J, Schein OD, Levy B, et al. A randomized trial of rigid gas permeable contact lenses to reduce progression of childrens myopia. Am J Ophthalmol 2003 Jul;136(1):82-90.
