Supplement to
| NEWS |
|
Check out more articles from the October issue of RCCL here! |
My Perspective: Failure to Communicate Practice Progress: Avoiding ‘Tunnel Vision’ Pharma Science & Practice: Red Alert Lens Care Insights: Mucin: Friend or Foe? Out of the Box: A Sticky Situation Features: Understanding Corneal Infection Care Keeping the Bugs at Bay: Fungi and Protozoa in Contact Lens Wearers How to Fend of Herpes and Varicella Zoster Considering Keratitis: Critical Question in Disease Management
|
| Have a topic you want to see discussed? Want to comment on an article? We want to hear from you! Contact us with your feedback and suggestions. |
20 Pearls on Corneal Infection Care As the number of contact lens wearers worldwide continues to increase, so too does the number of patients presenting with complex, sometimes treatment-resistant corneal infections. To help, the October issue of Review of Cornea & Contact Lenses is devoted to broadening your knowledge of the management of different corneal infections. Below are 20 pearls shared by several experts in the field. For more detail, click through to read the original articles for each. |
|
| |
| 2. Though controversial, adjunctive topical steroids can aid bacterial keratitis treatment. After 24 to 48 hours of antibiotic therapy, adding a topical steroid BID to QID can help speed resolution and possbily reduce corneal scarring. More
|
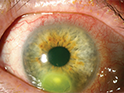
3. Because early Acanthamoeba keratitis often presents with a dendritiform or a nonspecific keratitis, two-thirds of these patients are misdiagnosed as having HSV keratitis. Pain out of proportion to clinical findings—a classic Acanthamoeba indication—can differentiate between the two. More |
|
4. For suspected or confirmed cases of Pseudomonas, gatifloxacin and ciprofloxacin provide better coverage than other FQs. Concomitant use of tobramycin or bacitracin/polymyxin B provides an even broader spectrum of coverage and further limits resistant bacteria. More
| |
| 5. In suspected infectious keratitis, obtain corneal scrapings for Gram stain and cultures with blood agar, chocolate agar, Sabouraud dextrose agar and thioglyoclate broth. Note, however, once the infection has advanced deeper into the stroma, a corneal biopsy may be necessary to confirm the diagnosis. More
| |
|
|
|
7. The clinical picture of herpetic uveitis can be quite variable: look for fine or granulomatous keratic precipitates that may be distributed diffusely, in Arlt’s triangle or in a linear pattern. Concomitant corneal edema, IOP spikes or sectorial iris atrophy may also appear. More
|
|
| 8. Treatment of isolated viral uveitis should include both oral antivirals at the correct treatment dosage for the suspected etiology, and a topical, and in some cases, oral corticosteroid to enhance penetration of medication into the anterior chamber. More
| |
| 9. When evaluating a patient for a bacterial infection, recording a thorough contact lens history, including nature and duration of symptoms, presence of discharge and changes in vision, can help pinpoint severity as well as identify more rapidly evolving infections. More
| |
| 10. Herpes viruses can remain dormant within the host and reactivate later; as such, these eyes must be treated over both the acute and chronic phase of the disease to prevent inflammation, scarring and a possible need for retransplantation. More
| |
| 11. Treatment should be tailored to the causal organism; however, in the case of a rapidly progressive disease process, patients cannot afford to wait until Gram stain results return. In these cases, consider first-line empiric treatment, which provides broad coverage against both Gram-positive and Gram-negative organisms. More
| |
|
|
| 13. Culture specimens should be obtained from the conjunctiva and lid margins of infected eyes, as well as from the leading edge and base of the corneal ulcer using a calcium alginate swap moistened with thioglycolate or trypticase soy broth. More
| |
| 14. In herpes zoster, dosing 400mg of acyclovir BID can reduce the rate of recurrent stromal disease—the manifestation most likely to lead to corneal transplant; however, long-term use can lead to acyclovir resistance, so only use the drug in cases that absolutely require it. More
| |
| 15. In cases of a corneal ulcer with corneal performation, consider amniotic membrane transplantation, which promotes re-epithelialization and inhibits inflammation. Use bandage contact lenses, autologous serum eye drops, punctal plugs or tarsorrhaphy to assist with healing. More
| |
| 16. Mild cases of adenovirus are self-limiting and can be treated using supportive means like chilled artificial tears, cool compresses and topical antihistamines; moderate to severe cases involving subepithelial infiltrates and symptomatic pseudomembrane formation should be managed using topical steroids. More
| |
|
17. Consider older, less frequently used drugs such as bacitracin, gentamycin and sulfacetamide for treatment-resistant corneal ulcers. For Gram-positive resistant bacteria, topical, fortified vancomycin can be used as a last resort. Be sure to tailor therapy as necessary using culture and sensitivity. More
| |
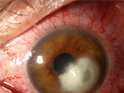
| 18. Fungal infections often have impressive anterior chamber inflammation with endothelial plaque and hypopyon. Despite this inflammation, they often have less lid edema and hyperemia than classically seen with bacterial infections. More | |
|
| |
|
19. Therapeutic PK can be used as a last resort in cases of corneal perforation or progressive corneal and scleral melt. Success of the graft is typically higher when the infection is localized and inflammation is controlled prior to surgery. More
| |
| |
|
| |
| |