| |
Volume 17, Number 2 |
June 2021 |
|
FROM
THE DESK OF THE EDITOR
Change is in the air. Restrictions are gradually easing up, allowing for some pre-pandemic normalcy to return. I just got back from a day of in-person continuing education. For the past 15 months, I’ve mostly done virtual with a few rare in-person lectures given masked (and yes, that was not pleasant). It was nice to have some social interaction with colleagues and actually get to see their unmasked faces. Don’t get me wrong, I’ve certainly enjoyed the virtual education as both a lecturer and an attendee. There is convenience and comfort in virtual education, avoiding the cost and time in traveling and enjoying the comfort of my home in my sweatpants. Everyone, whether you’re an adult or child, has a different learning style. A perfect world would offer a little bit of both platforms. We’ve certainly learned so much in the last 15 months as we’ve had to quickly pivot and adapt. I would love to see some positive change result from that. For CE, that will rely on our state licensing agencies to adapt to the times. Considering that, my optimism now takes a nose dive.
What else is in the air? Well, at my house it is cicadas….thousands of them. You know, the large insect with red, beady eyes that like to sing and shed their exoskeleton on trees and plants. Yep. My home in central Indiana appears to be in the epicenter of a plague of them. This particular species of cicadas comes out once every 17 years. My household went from trying to survive through a viral pandemic to avoiding a plague of bugs. Readers – I sure hope your summer has started off better than mine here in Indiana.
All the best! Cheers!
Anna Bedwell, OD, FAAO, FORS
Editor-in-Chief
PRESIDENT'S MESSAGE
Recently I was asked for a short writeup about ORS for one of the trade journals. The journal’s editor proposes a few questions, one of which was, “How was the society formed and how long ago?” I was dumbfounded by the fact that, as the current ORS President I did not know the answer to this question. So, the question became of interest to me as well. I emailed the eleven founding Fellows. The list of these esteemed colleagues can be found on ORS website. https://www.optometricretinasociety.org/about-us/
I received several replies and frankly learned a lot about the birth of the Optometric Retina Society. I hope in the future to make a chronicle and articulate the history I found so it can be posted in our website for the current and future members to learn this history. What I learned from this experience is how often we forget about the efforts of those who laid the foundation for the road we travel on.
I want to take this opportunity to thank all the eleven founding Fellows, particularly my two friends Bill Jones and Leo Semes who got me excited and involved in ORS. I apologize for not naming all the founding Fellows but encourage you to visit our website and see who these friends and colleagues are.
Mohammad Rafieetary, OD, FAAO, FORS
President, Optometric Retina Society

YOU
MAKE THE DIAGNOSIS
Answer appears later in newsletter.
Image Gallery
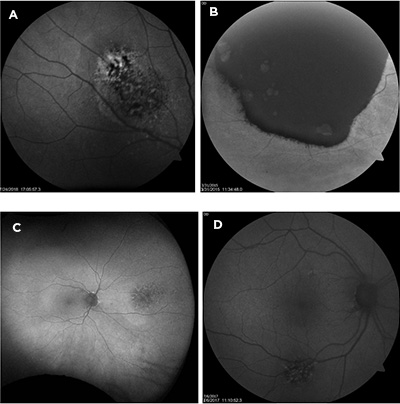
Which of the following fundus autofluorescence image shows a choroidal melanoma?
Answer appears later in the newsletter.
|
JOURNAL
ABSTRACTS
Intravitreal Aflibercept Injection vs. Sham as Prophylaxis Against Conversion to Exudative Age-Related Macular Degeneration in High-risk Eyes: A Randomized Clinical Trial
Once an eye with intermediate AMD converts to exudative AMD, the risk for conversion in the other eye becomes undoubtedly higher. For such high-risk eyes, could anti-VEGF injection serve as prophylaxis? This question was explored in a prospective, single-masked trial comparing intravitreal aflibercept injection (IAI) to sham injection. There were 128 participants across four sites randomized to quarterly treatment with either IAI or sham over 24 months. The participants all had exudative AMD (active or old) in one eye and intermediate AMD in the study eye, confirmed by the Boston Imaging Reading Center.
At study completion, 6 eyes (9.5%) in the IAI group and 7 (10.9%) in the sham group converted to exudative AMD. The majority converted within the first 12 months, 4/6 IAI group and 6/7 in the sham group. Conversion rate was higher in eyes whose fellow eye was diagnosed ≤2 years from study enrollment compared to eyes diagnosed longer ago. Of note, the rates of conversion were lower than expected for both groups (assumed 35% conversion). Unfortunately, IAI treatment did not demonstrate a protective effect and hence was not recommended to reduce conversion from intermediate to exudative AMD. Further investigation is necessary for a means to protect the vision in these high-risk eyes.
Heier JS, Brown DM, Shah SP, et al. Intravitreal Aflibercept injection vs sham as prophylaxis against conversion to exudative age-related macular degeneration in high-risk eyes: a randomized clinical trial. JAMA Ophthalmol. 2021 Mar 18:e210221. [Epub ahead of print].
Need for Retinal Detachment Reoperation Based on Primary Repair Method Among Commercially Insured Patients, 2003-2016
There are several treatment options when repairing a rhegamatogenous retinal detachment (RRD). While these procedures are often successful, none are 100% and may require further operation. This retrospective cohort study analyzed insurance claims, commercial and Medicare Advantage, for patients who underwent primary RRD repair to assess characteristics of those requiring reoperation. A two-year look-back was performed to ensure exclusion of patients with prior RD repair, determine clinical characteristics and exclude confounding ocular conditions (proliferative retinopathy, central serous chorioretinopathy, chorioretinitis, etc.). Only patients with three or more years of continuous enrollment in their health insurance plan were included.
From 2003 to 2016, a total of 16,190 cases of primary RRD repair met the inclusion criteria. Of those, 2,918 (18%) necessitated reoperation within 90 days of the initial procedure. A primary pneumatic retinopexy (PR) necessitated the most second procedures at 28.7% of cases, followed by scleral buckle (SB) at 19.1% and pars plana vitrectomy (PPV) at 17.9%. Primary laser barricade cases had the lowest likelihood of reoperation, likely attributable to less severe cases. Males were at greater odds (p<0.001) over females for needing a second repair. Other ocular co-morbidities included pseudophakia (p=0.001) and vitreous hemorrhage (p=0.001). PPV was elected most often as a secondary procedure.
This study gave real-world data on success rates for RRD repair. While the benefit to using insurance claims is certainly a robust sample size, the limitation is the lack of clinical information otherwise found in a patient record. Nevertheless, the authors found that almost one in five patients necessitated a second operation for RRD repair in the first 90 days. Of particular note, the success rate for a single operation for PR was lower than previous reports.
Reeves MG, Afshar AR, Pershing S. Need for retinal detachment reoperation based on primary repair method among commercially-insured patients, 2003-2016. Am J Ophthalmol. 2021; Apr 22. [Epub ahead of print].
Pneumatic Retinopexy vs. Scleral Buckling in Retinal Detachments with Superior Breaks: A Comparative Analysis of Outcome and Cost
In certain instances, involving retinal detachment with superior breaks, surgeons have a choice between pneumatic retinopexy (PR) and scleral buckling (SB) for repair. Pneumatic retinopexy can offer several potential advantages if it is a viable option for a given patient, such as being able to be performed in office, and not inducing the myopic shift that is common post SB. In this article, a tertiary retinal care facility in India retrospectively compared the results of patients with superior breaks who underwent PR to those with superior breaks who underwent SB over a four-year period. To be included in the review, the breaks must have been located in the superior portion of the fundus between 10-2 o’clock, and they could be no larger than one clock hour. Patients were excluded if they had a history of trauma, were less than 18 years old, had PVR worse than grade “B”, or were followed up for less than three months. Overall, 15 patients who underwent PR with C3F8 gas and 17 patient who underwent SB were included in the evaluation. With the exception of three patients in the PR group, all patients had a macula-off RD. Retina reattachment was achieved with the primary surgery in 66.7% of PR cases and 76.5% of SB cases, which was a statistically significant difference. Five eyes in the PR group and four eyes in the SB group had failed primary procedures. Final best-corrected visual acuity was 0.3 logMAR in the PR group and 0.75 logMAR in the SB group, with the difference not reaching statistical significance. The three-month cataract progression rate was similar between the two groups. Importantly, PR was six times faster and 50% less expensive than SB, giving it substantial practical advantages over SB in circumstances where its use is appropriate. This can be particularly important in developing countries.
Singh A, Behera UC. Pneumoretinopexy versus scleral buckling in retinal detachments with superior breaks: A comparative analysis of outcome and cost. Indian J Ophthalmol. 2021 Feb;69(2):314-8.
Real World Evidence on 5661 Patients Treated for Macular Oedema Secondary to Branch Retinal Vein Occlusion with Intravitreal Anti-vascular Endothelial Growth Factor, Intravitreal Dexamethasone or Macular Laser
Branch retinal vein occlusion (BRVO) is the second most common retinal vascular disease behind only diabetic retinopathy. The main cause of vision loss in patients with BRVO is macular edema. While anti-VEGF injection is the treatment most commonly undertaken, grid laser therapy and intravitreal steroid implants also have a role in certain patients. This review of 5,661 patients in England treated for BRVO-induced macular edema between 2002 and 2017, evaluated the real-world effectiveness of these various treatment modalities. Due to the tightly controlled nature of clinical trials, it is not uncommon for treatment modalities to perform better in trials than they do in real-world clinical practice. Patients across the three treatment groups were similar in age, had a similar gender mix and a similar ethnic mix. The mean initial baseline visual acuity was highest for the laser-treated patients and lowest for the patients treated with steroid implants. Patients who underwent anti-VEGF injections or steroid implants exhibited less visual acuity improvement than did patients who received those interventions in clinical trials. The treatment burden and number of visits were considerably higher for anti-VEGF injections than laser therapy or steroid implants, but the gain in visual acuity at 36 months was the greatest with anti-VEGF therapy. The average number of treatments at 36 months was 6.9 for anti-VEGF injections, 1.2 for laser, and 1.7 for steroid implants. Laser-treated patients actually experienced worse visual acuity at 36 months on average than they had at baseline, while anti-VEGF patients gained 11 ETDRS letters and steroid implant patients gained nearly 10 ETDRS letters.
Gale R, Pikoula M, Lee AY, et al; UK EMR Users Group. Real world evidence on 5661 patients treated for macular oedema secondary to branch retinal vein occlusion with intravitreal anti-vascular endothelial growth factor, intravitreal dexamethasone or macular laser. Br J Ophthalmol. 2021 Apr;105(4):549-54.
Retinal Vascular Manifestations of Obstructive Sleep Apnea
OSA is a disorder that is widely underdiagnosed with the potential for serious and/or visual threatening consequences. A recent meta-analysis found that patients with diabetes and OSA are more at risk for developing retinopathy. This realization has to do with several factors. The first is a sleep biomarker—apnea-hypopnea index (AHI), which is the number of apneic or hypoxic events per hour of sleep. The higher the AHI, the more likely the patient is to develop retinopathy or progress from non-proliferative (NPDR) to proliferative retinopathy (PDR). The second risk factor is circadian locomotor output cycles kaput (CLOCK) genes. OSA is known to dysregulate CLOCK genes. One CLOCK gene in particular is called DEC2, which is responsible for vascular endothelial growth factor (VEGF) expression. DEC2 is known to be upregulated in patients with OSA, again leading to increased risk of progression from NPDR to PDR. The impact of not treating OSA in patient that have diabetes is two-fold: Those patients are more at risk for developing retinopathy and the treatment used to combat that retinopathy is much less effective.
Retinal vein occlusion (RVO) trails diabetic retinopathy as the second most common retinal vascular disease. RVOs are linked to hypertension but recent research suggests a direct link between RVO and OSA. When a patient stops breathing due to OSA, the body experiences a state of hypoxia, hypoxic episodes increase the risk of a vaso-occlusive event—because when the body is starved oxygen sympathetic activity increases—peripheral vasculature constricts and oxidative stress can occur. The events just listed can result in venous stasis and endothelial damage, which increase the chances for thrombosis. The AHI is also related to RVO. As the AHI increases, the vascular caliber decreases and the pulse amplitude in those attenuated vessels increases, again increasing the risk for occlusive events.
Another vision-threatening condition is central serous chorioretinopathy (CSCR). Although studies show that male sex, age, and steroid exposure are still the strongest risk factors, OSA does impose an increased risk of developing CSCR. OSA increases levels of epinephrine and cortisol circulating in the body because of associated increase in sympathetic activity. A review of 10,753 patients with OSA and 322,590 controls patients shows that patients with OSA had a higher incidence of CSCR. The inverse was also true; patients with CSCR were more likely be diagnose with OSA.
OSA is a dangerous condition that can lead to mood disorders, cardiovascular disease, cognitive dysfunction, diabetes mellitus, and vision-threating retinal complications. It is important that eye care professionals pay attention to symptoms associated with OSA so patients can be referred for diagnosis and treatment and therefore decrease the risk of developing retinal vascular complications.
D'Souza H, Kapoor KG. Retinal vascular manifestations of obstructive sleep apnea. Curr Opin Ophthalmol. 2020 Nov;31(6):508-13.
Early Experience with Brolucizumab Treatment of Neovascular Age-Related Macular Degeneration
This retrospective case series focused on the outcomes and ocular safety of the newest anti-VEGF injection, brolucizumab. Brolucizumb was approved for use by the FDA in 2018 and by the European Medical Agency in 2020. This study follows 172 eyes with neovascular AMD in 152 patients over a total of 48 weeks. More than half (65.7%) of the eyes treated in this study had prior anti-VEGF treatment which had failed to resolved fluid.
All patients were treated with 6mg of brolucizumab via intravitreal injection (IVI). Of the 172 eyes studied, 105 eyes only received one injection, 55 eyes received two injections, and 12 eyes received three injections. The initial setup of the study called for an assessment of each patient after three loading doses given one month apart, but due to COVID-19, the study design had to be altered. Despite the design change, the study was still able to show that brolucizumab works at least as well as aflibercept.
Overall, there were no changes in the mean visual acuity of participants, and the mean central subfield thickness (CST) decreased. The mean CST was 296.7 microns in 151 eyes before starting brolucizumab, and the mean CST was 269.8 microns in the 144 eyes assessed at the last follow-up. The authors point out that a majority of the study participants were switched to brolucizumab, not to improve visual acuity, but because other drugs failed to eliminate retinal fluid. It is important to note that 44.2% of eyes had resolution of fluid with only one IVI of brolucizumab, and an additional 5.3% had resolution after two IVI.
However, there are ocular inflammation concerns with brolucizumab. Intraocular inflammation (IOI) developed in 8.1% of the eyes treated. One eye developed endophthalmitis and was successfully treated with intravitreal vancomycin. Of the eyes that developed IOI, most cases were mild and some resolved without intervention. One case, however, was severe and even with treatment resulted in occlusive retinal vasculitis. It appears that female sex and getting bilateral same-day brolucizumab are associated with an increased risk of IOI.
This study has limitations: Only four of the eyes treated were treatment-naive and in the group that had received previous treatments, those treatments varied greatly. There was also no control group, which makes it difficult to compare this study directly to previous studies of the same nature. Despite the limitations, this study was able to confirm the efficacy of brolucizumab as a treatment option for nAMD. The incidence of IOI for brolucizumab was 4.4% per injection compared to 2.9% for other anti-VEGF treatment options, which should be taken into consideration.
Enríquez AB, Baumal CR, Crane AM, et al. Early experience with brolucizumab treatment of neovascular age-related macular degeneration. JAMA Ophthalmol. 2021 Apr 1;139(4):441-8.
|
ANSWER
TO "YOU MAKE THE DIAGNOSIS"
Adult-onset Foveomacular Vitelliform Dystrophy
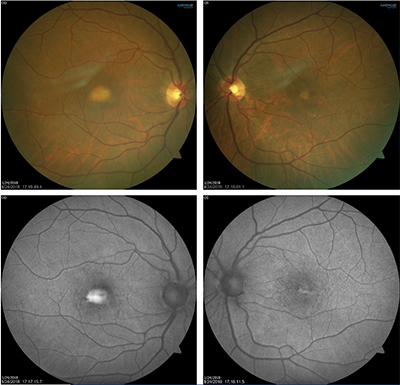
A 63-year-old Caucasian female presented for routine exam with mild near vision complaints. Her medical history was significant for hypertension. The patient had been told by past eye doctors that she had macular degeneration.
Best-corrected visual acuities were 20/30 right eye and 20/20 left eye. Preliminary testing was unremarkable. On exam, she had grade 1 nuclear sclerotic cataracts in both eyes. Fundus exam, as seen in images above, showed bilateral subfoveal yellow lesions in each eye with the right larger than the left. On fundus autofluorescence, the right eye lesion was brightly hyperfluorescent while the left eye showed mixed hyper and hypofluorescence. SD-OCT (Figure 3, below) was obtained, and revealed the lesions were mostly hyperreflective and located subretinal, below the ellipsoid zone. Additionally, the scans showed vitreomacular adhesion without traction, unrelated to the subretinal lesions. Based on this testing, the patient was diagnosed with adult-onset foveomacular vitelliform dystrophy. There was no evidence of age-related macular degeneration.
Adult-onset foveomacular vitelliform dystrophy (AFVD) is categorized as one of the pattern dystrophies. The inheritance pattern of AFVD is unclear and has been associated with mutations in PRPH2, BEST1, IMPG1 and IMPG2 genes.1 Clinical features of AFVD typically onset in middle age.1 The characteristic appearance is bilateral foveal lesions one-third to one-half disc diameters in size and yellowish in color.2,3 Though over time, the yellow lesions can fade or RPE atrophy can develop. With its pathognomonic features, OCT can aid in proper diagnosis. AFVD lesions are located below the sensory retina, between the ellipsoid zone and RPE.4 The lesions are mostly hyper-reflective, though there may be some hypo-reflectivity.4 On fundus autofluorescence (FAF), there is generally hyperfluorescence corresponding to increased levels of lipofuscin.5 But the FAF pattern can be variable and change over time, particularly in the late stage as atrophy develops.5
The clinical appearance of AFVD closely resembles that of Best’s disease. However, disease onset and diagnostic testing will differ between them. Best’s disease typically onsets during childhood, has much larger vitelliform lesions than in AFVD and on EOG will be severely reduced. Likewise, AFVD can be mis-diagnosed as macular degeneration as was seen here. Thorough testing with OCT and FAF can help to differentiate the two, though some AFVD patients can also develop AMD.
Symptomatology of AFVD varies, with some patients completely asymptomatic.1 Others will report blurring of vision or metamorphopsia. Vision loss is generally mild early on in the disease and progresses slowly. There is no treatment for AFVD. Patients should be monitored for development of choroidal neovascular membrane, though occurrence is relatively uncommon.
Anna Bedwell, OD, FAAO, FORS
Editor-in-chief
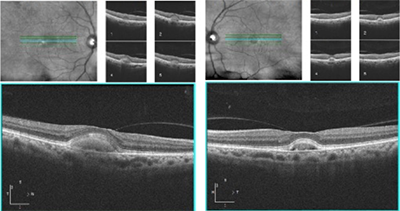 |
| Figure 3: OCT images of both eyes showing hyperreflective lesions at the fovea. The lesions are located below the ellipsoid zone, consistent with a diagnosis of adult-onset foveomacular vitelliform dystrophy. |
References:
1. Chowers I, Tiosano L, Audo I, et al. Adult-onset foveomacular vitelliform dystrophy: A fresh perspective. Prog Retin Eye Res. 2015 Jul;47:64-85.
2. Gass JDM. A clinicopathologic study of a peculiar foveomacular dystrophy. Trans Am Ophthalmol Soc 1974;72:139-56.
3. Epstein GA, Rabb MF. Adult vitelliform macular degeneration: diagnosis and natural history. Br J Ophthalmol 1980;64(10):733-40.
4. Puche N, Querques G, Benhamou N, et al. High-resolution spectral domain optical coherence tomography features in adult onset foveomacular vitelliform dystrophy. Br J Ophthalmol 2010;94:1190-1196.
5. Parodi MB, Iacono P, Pedio M, et al. Autofluorescence in adult-onset foveomacular vitelliform dystrophy. Retina. 2008;28(6):801-7. |
IN THE
NEWS
|
 NEI Launches AREDS2 Data Access for New Research NEI Launches AREDS2 Data Access for New Research
The NEI Data Commons recently added AREDS2 data access for research. The AREDS2 database includes participant data (demographics, diet and eye health) and stem cell lines, which were developed in collaboration with the New York Stem Cell Foundation Research Institute (NYSCF). For researchers, this will provide AMD models with various genetic backgrounds to gain a better understanding of the disease. There are over 60 NYSCF pluripotent stem cell lines accessible with plans to add accompanying genomic and phenotypic data including retinal images of participants. Researchers must submit a research proposal and sign an agreement to gain access to the database.
|
|
J&J Receives FDA Approval for Acuvue Abiliti
Orthokeratology (ortho K) contact lenses have long been an off-label tool utilized to curb myopia progression, until now. J&J recently announced FDA approval of an ortho K lens specifically for myopia management. J&J collaborated with Menicon to design this therapeutic rigid lens worn overnight under the brand name Acuvue Abiliti Overnight. Abiliti utilizes a fitting software program that combines the corneal measurements and refractive error to help streamline the fitting process. The lens also has a toric option, Abiliti Overnight for Astigmatism. J&J expects Abiliti to be available in the US by the end of 2021.
|
|
FDA Grants Clearance for MedOne Surgical’s MicroDose Injector
MedOne Surgical announced FDA 510(k) of its MicroDose Injector. The injector is designed for low volume subretinal injections. It is pneumatically driven, utilizing a vitrectomy system. The pneumatic design provides better surgeon control over a manual injection. MicroDose Injector is compatible with multiple vitrectomy systems and available for commercial order. |
|
Novartis Calls Off Three Beovu Trials Prompted by Year One MERLIN Results
Novartis announced year one results of the MERLIN study, a two-year Phase III study of Beovu (brolucizumab) 6 mg in exudative AMD patients with persistent retinal fluid. In comparison to 2 mg aflibercept, Beovu proved non-inferiority in change in visual acuity from baseline and superiority in select secondary anatomic outcomes. However, a higher frequency of intraocular inflammation (IOI) adverse events (including retinal vasculitis and retinal vein occlusion) was found in the Beovu 4-week dosing group (9.3% vs 4.5% in aflibercept 4-week dosing). Out of safety concerns, the IOI events prompted Novartis to terminate the MERLIN trial as well as RAPTOR and RAVEN. Other trial protocols have been modified to discontinue 4-week dosing after the loading phase. Per Novartis, physicians should not administer Bevou 6 mg at intervals less than 2 months once beyond the loading phase.
|
| |
Notal Vision Secures Financing to Support Home OCT Device
Notal Vision, Inc. announced closing of a Series D financing in support of the company’s Foresee Home AMD Monitoring Program and Home OCT technology. The financing, a total of $60 million, was co-piloted by Soleus Capital and Ganot Capital, Notal Vision’s majority shareholder, with contribution from existing shareholders Elron and Evergreen.
|
|
Nanoscope Reports Vision Improvement in Optogenetic Gene Therapy Trials
Nanoscope Therapeutics announced positive one-year results from its Phase I/IIa optogenetic gene therapy trial. The trial consisted of 11 severe retinitis pigmentosa cases of various genetic mutations. Subjects received gene therapy of multi-characteristic opsin delivered by retinal injection with an adenoviral virus vector. Three received low-dose (1.75 x 1011 VG) treatment and eight high dose (3.5 x 1011 VG). Six of the seven high-dose patients that completed one-year follow-up, gained over 15 letters of vision. Subjective and objective functional vision improvement was noted in all participants. Nanoscope plans to start a Phase IIb trial this summer.
|
|
IMAGE QUIZ ANSWER
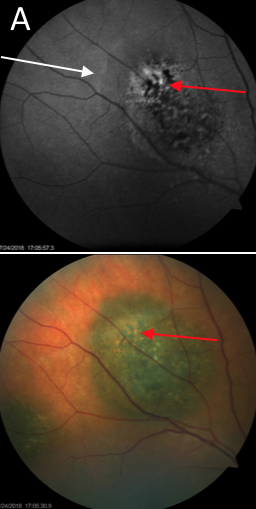
Image A is a fundus autofluorescence (FAF) image of a choroidal melanoma. Both the FAF and color image are shown on the left. In the color image, the red arrow points to orange pigmentation, which is lipofuscin. This is brightly hyperfluorescent on the FAF image. The white arrow denotes a mildly hyperfluorescent ring around the melanoma, corresponding to the leading edge of subretinal fluid.
Recently, there has been an increased emphasis on using imaging techniques, such as OCT and FAF, to monitor choroidal nevi for transformation to melanoma. FAF, specifically, can be used to screen for lipofuscin, a risk factor for malignancy.
B: CHRPE C: choroidal nevus with drusen
D: choroidal nevus with drusen
|
WHY BECOME AN ORS FELLOW?
By Bill Denton, O.D., F.A.A.O.
Chair, Membership Committee
At some point in your career, you realize you just may be coasting. Your knowledge has been limited to the journals you receive and attempt to read, and the conferences that may not be as fulfilling as they once were. You simply need a challenge that will add an extra dimension to your professional learning.
Fellowship in the Optometric Retina Society (ORS) can provide several benefits in addition to the initial challenge of qualifying for this honor. Plenty of perks accompany your induction, but the coolest part is being associated with a body of knowledge and resources which can help you in many other ways. It is not uncommon to receive weekly thought-provoking emails about challenging cases and treatment dilemmas. Some fellows like to share their awesome cases they have diagnosed, while others post their cases with hopes that other Fellows will suggest an alternative differential diagnosis. At times it is like a round-table of brainstorming, but through the use of modern technology. Fellowship has little obligation with a huge opportunity for professional growth.
If you are up to the challenge of becoming a Fellow of the ORS, feel free to peruse the details and application at www.optometricretinasociety.org. Advice can be given to assist you in your quest. Feel free to contact us.
|
Editor
in Chief
Anna K. Bedwell, OD, FAAO
Co-Editor
Brad Sutton, OD, FAAO |
Journal
Reviewers
Meret Thomas-Huebner, OD
Senior Graphic Designer
Matt Egger
|
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 11 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|