| |
Volume 18, Number 2 |
June 2022 |
|
FROM
THE DESK OF THE EDITOR
Summer is here! A heat wave hit my midwestern home last week and now it officially feels like summer. If you likewise attended Optometry’s Meeting in Chicago last week, then you certainly felt it as well! I’m going to keep this message short. Between work and summertime excursions, it’s been extra busy.
There is a lot of great content to share below. Of particular interest to me was reading the ALOFT study looking at long-term data of the ForeseeHome, a home monitoring service to detect conversion to neovascular AMD. It may have particularly peaked my interest because my office recently started using it in our practice for high-risk intermediate AMD patients. The results were impressive, showing patients were able to maintain a much better visual acuity than without the device. As more emphasis goes into artificial intelligence devices, like ForeseeHome and home-based OCT monitoring, I’m interested to see where we are 10 years from now and what effect will home based monitoring have on retina care. We’ll see. For now, stay cool and enjoy the summer weather.
Cheers!
Anna Bedwell, OD, FAAO, FORS
Editor-in-Chief
PRESIDENT'S MESSAGE
It is hard to believe 2022 is half over! I hope this message finds you healthy, happy, and in good spirits. From the looks of public places, airports, and the comeback of our profession’s in-person meetings, our lives are slowly normalizing. If you haven’t yet, check out the 2022 ORS Resident Case Report Contest in the June issue of Review of Optometry. It is so wonderful, beyond two excellent case reports by two bright optometric residents, to see the desire of the “new blood” to move optometry forward, while at the same time reflecting on how we have stood on the shoulder of icons such as Larry Alexander, who paved the road. Congratulations to Claire Cordoba, OD, a primary care resident at the Indiana University School of Optometry, and Keying Yan, OD, ocular disease resident at the BronxCare Health System in New York, and praises to Dr. Julie Rodman and our other colleagues who have played instrumental roles to keep this contest going.
We are planning the ORS Retina Update meeting December 10-11 at the Hilton Jolla Torrey Pines, in La Jolla, California. Hope to see all you there.
Have a great summer and be safe.
Mohammad Rafieetary, OD, FAAO, FORS
President, Optometric Retina Society

ORS Announces Larry Alexander Case Report Winners
The ORS is pleased to announce the winners of the sixth annual Larry Alexander Resident Case Report Contest. The contest was sponsored by Topcon, Visionix (Optovue) and Heidelberg. The case reports are available to read online at: https://www.reviewofoptometry.com/
The co-winners are:
Claire Cordoba, OD, a primary care resident at the Indiana University School of Optometry - Bilateral Bartonella Henselae Neuroretinitis
Keying Yan, OD, an ocular disease optometry resident at the BronxCare Health System in New York – Detecting and Managing Multifocal Vitelliform Dystrophy
|
YOU
MAKE THE DIAGNOSIS
Answer appears later in newsletter.
Image Gallery
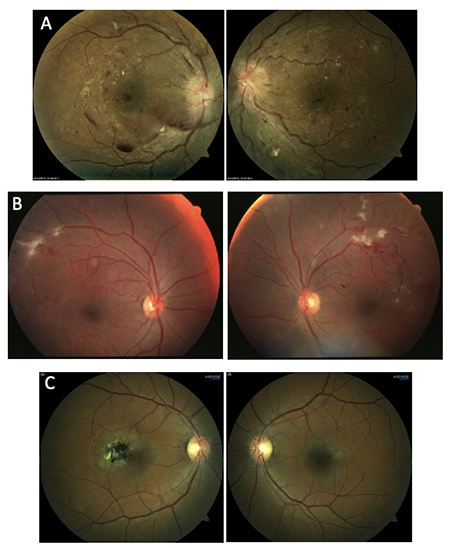
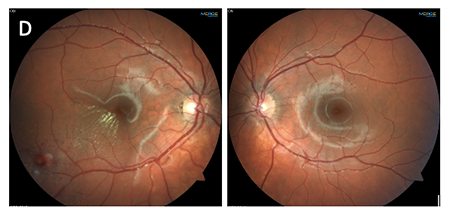
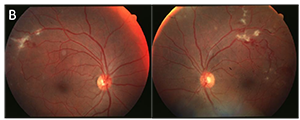
Which of the following images represents Eales’ disease?
Answer appears later in the newsletter.
|
JOURNAL
ABSTRACTS
Retinal Detachment After Cataract Surgery: a Population-based Study
Rhegmatogenous retinal detachment (RRD) is one of the most significant complications associated with cataract surgery, carrying with it a risk of permanent visual impairment. The overall risk of RRD after cataract surgery has been reported at .2% to 3.6% in the literature. When discussing potential cataract surgery with patients, it is imperative to include the postoperative increased risk of retinal detachment in that discussion. It is particularly important to understand which types of patients are at the highest risk and counsel them appropriately. This study from Sweden contains some very interesting conclusions regarding who those patients are. It reviewed over 58,000 cataract surgery cases performed over a three-year period with average follow-up time of 4.67 years. The investigators considered many variables, but three ultimately proved to be important: sex, age, and axial length. Patients were broken down by male vs. female, axial length (<23mm, 23 to 25, >25) and age (<60 years, 60 to 75, >75). Overall, the rate of RRD was found to be 2.4% for those under 60 years old, .65% for those 60-75, and .17% over 75 years old. When evaluating by axial length, the risk was .11% under 23 mm, .39% from 23 to 25mm, and 1.86% over 25mm. Of all the RRD cases, 68.8% were male.
These statistics, though they may not be fully applicable across different patient populations, offer some very valuable insight into RRD risk after cataract. Perhaps the most striking finding is that males under 60 years old with an axial length >25mm had a 9.46% risk of RRD. Thus, nearly one in 10 patients who fit those criteria suffered an RRD after cataract surgery. Conversely, patients over 75 years old had an extremely low overall risk of RRD, even if they were male and highly myopic. Clearly, younger patients who are male and highly myopic have a much higher risk of RRD after cataract surgery than the typical risk relayed to patients when discussing cataract surgery, and patients over 75 years old have an extremely low risk. When discussing surgical risks with individual patients, these factors should be considered.
Thylefors J, Jakobsson G, Zetterberg M, Sheikh R. Retinal detachment after cataract surgery: a population-based study. Acta Ophthalmol. 2022; Mar 25. [Epub ahead of print].
Effect of Surgical Timing in 23-g Pars Plana Vitrectomy for Primary Repair of Macula-off Rhegmatogenous Retinal Detachment, a Retrospective Study
When an eye has experienced rhegmatogenous retinal detachment (RRD), several factors are involved in ultimately determining long term visual potential. One of the most important of those factors is the status of the fovea, with it being “on” or “off” at the time of repair. Fovea-on retinal detachments are emergent situations, with repair being undertaken as soon as possible in an attempt to preserve central visual function. When a patient reports with a fovea-off RRD, however, there is far less consensus regarding the timing of repair. This retrospective study, which was performed at the University of Virginia, examined the effect of delayed repair in patients with fovea-off RRD. Only patients who were repaired utilizing 23-gauge vitrectomy were enrolled. Those who were repaired with pneumatic retinopexy, scleral buckle, or 25-/27-gauge vitrectomies were excluded. Those with bilateral detachments, those with repeat detachments, those who were not followed for at least six months, and those under 18 years of age were also excluded.
A total of 104 patients who underwent 23-gauge vitrectomy between July 1, 2012 and July 1, 2020, were enrolled. They were divided into three groups based upon the perceived duration of foveal detachment related central vision loss: less than 48 hours, 3 to 7 days, and greater than seven days. There was no significant difference in the final logMAR visual acuity at the final visit in the early repair group (.28) and the moderately delayed repair group (.35). However, the final visual acuity was significantly worse (.90) in the late repair group. Interesting, the re-detachment rate was 26% in the early repair group, 17% in the moderately delayed group, and a substantial 56% in the late repair group. In total, 22 of the 104 patients experienced re-detachment during the study period. This study seems to indicate that patient outcomes are not affected by a delay of up to 7 days when repairing fovea-off RRD’s. After a delay of seven days or more, however, final visual acuity is substantially decreased on average and the rate of re-detachment is over 50%.
While this is important and valuable information, there are some important caveats to consider. The study only looked at repair with 23-gauge vitrectomy, with other methods of repair being excluded. Therefore, these findings may not apply to repair with scleral buckle, etc. Also, the period of delay in repair does not likely have a hard cutoff when it comes to outcomes. For example, the range of delay in the late repair group was 10 to 180 days. It would be reasonable to assume that a patient with delay of 10 days may do just as well as a patient with a delay of 7 days, though they fall in different study groups, while a patient with a delay of 180 days almost certainly will not have a good outcome.
Elghawy O, Duong R, Nigussie A, et al. Effect of surgical timing in 23-g pars plana vitrectomy for primary repair of macula-off rhegmatogenous retinal detachment, a retrospective study. BMC Ophthalmol. 2022; Mar 25;22(1):136.
Current Practice in the Management of Ocular Toxoplasmosis
The purpose of this study was to define current practice methods for the diagnosis and treatment of ocular toxoplasmosis. There were 192 study members that participated in a 36-item survey on the clinical features, use of investigations, indications for treatment, systemic and intravitreal treatment with antiparasitic drugs and corticosteroids, and approach to follow-up and preventative therapy. Each study member was a uveitis-specialized ophthalmologist. Most study members reported that their patients had typical disease (unilateral, retinochoroiditis at the border of a pigmented scar), but atypical disease was encountered by over half of the study members. An atypical clinical presentation was more common in individuals who were immunocompromised, elderly, or those receiving chronic corticosteroid injections, but one-third of members also noted atypical presentation in healthy individuals. Clinical examination along with T. gondii serology was used to diagnose ocular toxoplasmosis by 56.8% of members in typical cases, while 35.9% relied on clinical examination alone for diagnosis. In atypical case presentations 68.9% of members included intraocular fluid testing, 53.6% tested aqueous, 22.4% tested vitreous, and 9.4% tested both to aid in diagnosis. DNA polymerase chain reaction (PCR) was favored by members over T. gondii antibody-based Goldmann-Witmer coefficient testing.
The majority of members (66.1%) treated all non-pregnant patients at presentation, while most (74.0%) did not treat every pregnant patient. Systemic trimethoprim-sulfamethoxazole was preferred as first-line therapy by 66.7% of members, 60.9% used it alone, while 39.0% used it in combination with other medications. Treatment with intravitreal clindamycin was used by 96.7% of study members, and systemic corticosteroid treatment was used by 97.4%. Only 43.2% of study participants treated every patient with systemic corticosteroids, while 55.7% used them selectively. Intravitreal corticosteroid injections were only used by 24.7% of members and were almost always given in conjunction with an intravitreal antimicrobial drug. The majority of members (60.4%) continued to follow patients after resolution of active ocular toxoplasmosis, and trimethoprim-sulfamethoxazole was the most common (92.4%) agent used for prophylaxis against recurrent infection. These results can be used as a guide for testing, treatment, and follow-up of ocular toxoplasmosis patients.
Yogeswaran K, Furtado JM, Bodaghi B, et al; International Ocular Toxoplasmosis Study Group. Current practice in the management of ocular toxoplasmosis. Br J Ophthalmol. 2022; Feb 23. [Epub ahead of print].
Predictors of Myopia Macular Degeneration in a 12-year Longitudinal Study of Singapore Adults with Myopia
This 12-year, prospective longitudinal study aimed to investigate the predictive factors for myopic macular degeneration (MMD) and progression of MMD in adults with myopia. Participants were 40 to 80 years old, and 1504 myopic eyes without MMD were included in the study. Another 75 eyes with MMD at baseline were included to assess progression over the 12-year period. Previously known risk factors associated with MMD include older age, greater myopic spherical equivalent (SE), and longer axial length (AL). Refraction, AL using non-contact partial coherence interferometry, and color fundus photography after cycloplegia were obtained on all subjects at baseline and repeated at the 12-year follow-up. The 12-year cumulative MMD development of 1504 myopic eyes without MMD at baseline was 10.3% (155 eyes). Of the 155 eyes, 127 (81.9%) had a tessellated fundus at baseline. Patients who were older (≥60 years old) and had a tessellated fundus at baseline had a higher incidence (34.9%) of MMD development over the 12-year period. A higher incidence (47.4%) of MMD development was seen in those with high myopia and tessellated fundus. The 12-year cumulative progression in the 75 eyes with MMD at baseline was 12.0% and the highly myopic eyes (≥-5.00 diopters) had a progression rate of 19.6%. Overall, it was found that older individuals with tessellated fundus and high myopia were more likely to develop MMD over time compared to other subgroups and should be monitored more closely.
Foo LL, Xu L, Sabanayagam C, Htoon, et al. Predictors of myopic macular degeneration in a 12-year longitudinal study of Singapore adults with myopia. Br J Ophthalmol. 2022; May 9. [Epub ahead of print].
Analysis of the Long-term Visual Outcomes of ForeseeHome Remote Telemonitoring (ALOFT)
The ForeseeHome (FSH) Monitoring Program is a monitoring approach for detection of neovascular macular degeneration (nAMD) utilizing an in-home device to measure a change in hyperacuity. Patients with intermediate AMD are trained to use the in-home device and a baseline is set. Telemonitoring is provided by the Notal Vision Monitoring Center.
The ALOFT study analyzed the long-term vision outcome of intermediate AMD eyes using FSH. This retrospective review used medical records from 5 referral clinics over the course of August 2010 to July 2020. A total of 2123 patients (3334 eyes) with established valid baseline test results were monitored with FSH. ALOFT followed eyes from baseline to time of conversion to nAMD, and final follow up. A total of 285 eyes converted to nAMD at an annual rate of 2.72% over the course of the study. A mean of 82 (±17.3) injections were given over a course of 2.7 (±2.0) years. Fifty-two percent of conversions were detected by an FSH alert, and the remaining were determined by symptoms or routine visit.
At the final study follow-up, 84% of eyes maintained vision of 20/40 or better. By contrast, only 34% of eyes maintain 20/40 or better from real-world IRIS data under standard of care. False positives, aka non-nAMD alerts, were infrequent and occurred on average once every 4.6 years per participant. The study boasted an impressive maintenance of VA for nAMD conversions. Of note, participants were very consistent in using the device, logging an average 5.2 tests per week consistently. These results are encouraging for intermediate AMD participants though a high level of commitment may be needed.
Mathai M, Reddy S, Elman MJ, et al; ALOFT study group. Analysis of the Long-term visual outcomes of ForeseeHome remote telemonitoring - The ALOFT study. Ophthalmol Retina. 2022; Apr 25. [Epub ahead of print].
Multimodal Assessments of Drusenoid Pigment Epithelial Detachments in the Age-Related Eye Disease Study 2 Ancillary Spectral-Domain Optical Coherence Tomography Study Cohort Summary
Drusenoid pigment epithelial detachments (DPEDs) are associated with an increased risk of progression to late-stage age-related macular degeneration (AMD), especially geographic atrophy. DPEDs are formed by soft drusen confluence and appear as large, yellow mounds measuring ≥433µm in diameter on fundus examination. They appear as retinal pigment epithelial (RPE) detachment composed of homogenous, hyperreflective material on optical coherence tomography (OCT). But little is known of their natural history.
This study was a retrospective analysis of study eyes from the AREDS2 Ancillary SD-OCT (A2A) study containing a DPED on CFP and confirmed by OCT on at least one follow-up. Thirty-one eyes were enrolled in this study and were followed over a median of four years. DPEDs were identified more frequently and earlier by OCT compared to CFP, with agreement of detection on both OCT and CFP in 50% of cases. By the time DPED was detected on CFP, OCT measured the average length of DPED as 4 times the diameter of 433µm used to define DPEDs on CFP. In cases where DPEDs were identified on CFP but not on OCT, OCT revealed non-DPED pathologies including epiretinal membrane, fibrosis, and acquired vitelliform lesions. This highlights the importance of utilizing OCT to identify these lesions, as DPEDs have different prognostic implications compared to the other lesions.
Of the eyes with DPEDs, 25% developed neovascular AMD, 29.2% underwent DPED collapse, and 45.8% had persistent DPEDs without progression to late-stage AMD. Eyes progressing to neovascular AMD had greater DPED lengths and heights preceding neovascularization, and those with greater DPED length progressed significantly faster than those with DPED collapse. Eyes that progressed to neovascular AMD and DPED collapse had hyperreflective foci (HFRF) over an area of RPE elevation. HRF detection preceded DPED growth and collapse by 19 months. Of DPED-collapsed eyes, 42.9% developed geographic atrophy formation. The mean time to DPED collapse was 3.9 years; Reduction in DPED size began 10 months before collapse.
DPEDs are common in AMD and can persist or collapse and lead to neovascular AMD and geographic atrophy. OCT can be used to confirm and monitor progression of DPEDs and identify high-risk features that correspond to progression.
Thavikulwat AT, De Silva T, Agrón E, et al; Age-Related Eye Disease Study 2 Ancillary Spectral Domain Optical Coherence Tomography Study Group. Multimodal assessments of drusenoid pigment epithelial detachments in the age-related eye disease study 2 ancillary spectral-domain optical coherence tomography study cohort. Retina. 2022;x May 1;42(5):842-851.
|
ANSWER
TO "YOU MAKE THE DIAGNOSIS"
Ischemic branch retinal vein occlusion with neovascularization of the disc and retina
A 41-year-old Native American female presented for a routine examination with near vision complaints. Her health history was remarkable for hypertension, depression, and anxiety for which she was taking losartan. Ocular history was unremarkable. Social history was significant for cigarette smoking.
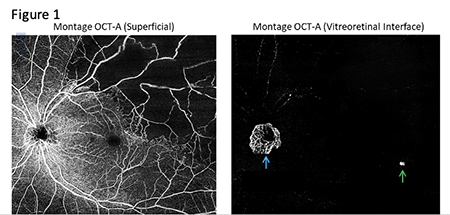
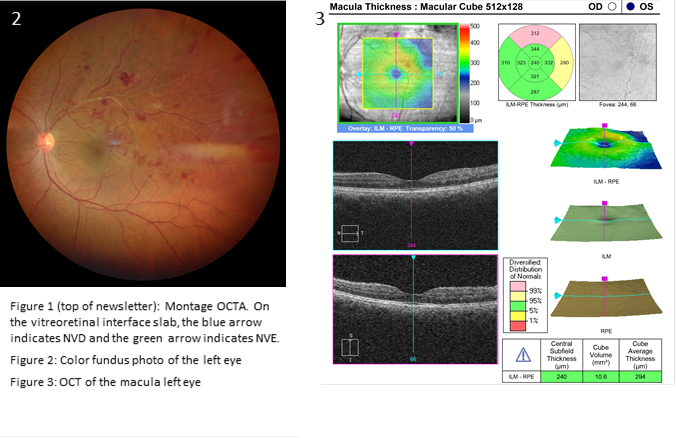
Best-corrected visual acuities were 20/20 right eye and 20/20 left eye. Entrance testing and anterior segment examination in both eyes was unremarkable. In-office blood pressure was 133/83. Intraocular pressures were 15 mmHg right eye and 16 mmHg left eye. The posterior segment of the right eye was unremarkable. Posterior segment examination of the left eye revealed multiple dot-blot and flame shaped hemorrhages in the superior temporal posterior pole adjacent to a sclerosed vein (Figure 2 below). Optical coherence tomography angiography (OCTA) (Figure 1 above) revealed greater than 5 disc diameters of retinal non-perfusion in the superior temporal posterior pole. No apparent macular ischemia was present, and the foveal avascular zone was normal in size and contour. The vitreoretinal interface preset enface OCTA also confirmed neovascularization of the disc (NVD) and a small area of retinal neovascularization elsewhere (NVE) temporal to the macula. Macular OCT (Figure 3 below) revealed minor, non-central macular edema in the superior temporal perifovea.
The retinal findings in the left eye demonstrated an ischemic branch retinal vein occlusion (BRVO) with NVD, NVE, and minor macular edema. Due to the patient’s young age, laboratory studies were ordered to rule out autoimmune or infectious etiologies including: CBC with differential, HbA1c, FTA-ABS, HIV, prothrombin time/partial thromboplastin time, ANA, rheumatoid factor, Factor XII, antiphosphatidylserine, antithrombin III, Factor V, homocysteine, protein S and protein C. The patient was referred to a retinal specialist and asked to follow-up in one month for gonioscopy and continued monitoring.
The laboratory testing came back normal for everything except elevated white blood cell count. Further investigation into the patient’s health history revealed uncontrolled hypertension with blood pressure readings of 147/110 and 136/96, 11 and 5 months prior to the ocular examination, respectively. Accordingly, the ischemic BRVO was suspected to be due to uncontrolled hypertension.
BRVO, the second most common retinovascular disorder, occurs due to blockage of a branch of the central retinal vein at an arteriovenous crossing.1 The superotemporal quadrant is most commonly affected and is seen in 63% to 66% of cases.2 Risk factors include: older age, hypertension, diabetes mellitus, glaucoma, hypercoagulability, oral contraceptives, and cigarette smoking.1,3
Patients with greater than 5 disc diameters of non-perfusion have a 36% risk of developing NVE or NVD and a 60% to 90% chance of developing a vitreous hemorrhage if laser photocoagulation is not performed.2 NVE, usually developing at the border of ischemic retina, is more common than NVD, both typically occurring 6 to 12 months after initial occlusion.3 Posterior segment neovascularization increases risk of vision-threatening sequelae including tractional retinal detachment, neovascular glaucoma, and vitreous hemorrhage.1 Neovascularization of the iris and neovascularization of the angle are less common in BRVO than CRVO, occurring in 2% to 3% of cases within 3 years.3 Initial treatment of macular edema and neovascularization secondary to BRVO typically includes sectoral panretinal photocoagulation and intravitreal anti-VEGF injections.1,3
Komal Patel, OD
Primary Care Resident
Oklahoma College of Optometry
Carolyn Majcher, OD, FAAO, FORS
Associate Professor
Oklahoma College of Optometry
References
1. Khayat M, Williams M, Lois N. Ischemic retinal vein occlusion: characterizing the more severe spectrum of retinal vein occlusion. Surv Ophthalmol. 2018; Nov;63(6):816-50.
2. Cochran ML, Mahabadi N, Czyz CN. Branch retinal vein occlusion. StatPearls: Treasure Island. StatPearls Publishing. 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK535370/.
3. Bowling B and Kanski JJ. Kanski's clinical ophthalmology: A systematic approach (8th ed). Elsevier. 2016:396-450.
|
IN THE
NEWS
|
 B&L and Clearside Announce Xipere Launch B&L and Clearside Announce Xipere Launch
Bausch + Lomb and Clearside Biomedical, a biopharmaceutical company developing suprachoroidal space drug delivery, reveal the launch of Xipere (triamcinolone acetonide injectable suspension) in the US. Xipere marks the first FDA-approved treatment with a suprachoroidal delivery approved for macular edema associated with uveitis. The SCS Microinjector® used to deliver the drug was developed by Clearside Biomedical.
|
|
NEI Researchers Report Novel Inherited Macular Dystrophy
A team of researchers from the National Eye Institute published a report in JAMA Ophthalmology (doi:10.1001/jamaophthalmol.2022.1822) identifying a newly discovered macular dystrophy. The dystrophy, of yet to be named, is caused by variants in the TIMP3 gene. Sorsby fundus dystrophy similarly is caused by a variant in the TIMP3 gene. The newly discovered dystrophy differed in clinical course and mechanism from Sorsby. In the report, two families were followed with an early-onset diffuse maculopathy that did not develop choroidal neovascularization.
|
|
FDA Grants Approval for Beovu in the Treatment of Diabetic Macular Edema
Novartis reported FDA approval for Beovu (brolucizumab-dbll) 6mg for the treatment of diabetic macular edema. This marks the second approved indication for the drug, which was initially approved for the treatment of wet AMD in 2019. Approval was based on data from two phase III studies, KESTREL and KITE. The approved prescribing for DME starts with a loading phase of five doses at q6 weeks followed by a dose q8-12 weeks. |
|
Opus Announces Collaboration with Resilience for Gene Therapy
Opus Genetics, a company focused on gene therapy for inherited retinal diseases and backed by Foundation Fighting Blindness’s venture arm, announced a manufacturing services agreement with National Resilience. (Resilience). Resilience is a biomanufacturing company dedicated to increasing access to complex medicine. In the agreement, Resilience will support the development and manufacturing of Opus’ pipeline of adeno-associated viral (AAV) vector-based gene therapies.
|
| |
Mireca Partners with Graybug Vision
Mireca Medicines announced in April its partnership with Graybug Vision to develop Mireca’s propriety treatment, cGMP analogues, targeting the treatment of inherited retinal disease. The partnership gives Graybug sole access to Mireca’s protein kinase G modulators. Graybug will be responsible for the research, development, manufacturing and commercialization of these cGMP analogues for the eye and ear disease treatment. In turn, Mireca will transfer to Graybug an Orphan Drug Designation for the treatment of retinitis pigmentosa.
|
|
|
|
IMAGE QUIZ ANSWER
Answer B represents Eales’ disease, an occlusive vasculitis. Eales’ most often affects young males of Middle Eastern descent. The clinical presentation is typically bilateral with a predilection for mid-peripheral and peripheral retina. The early stages are characterized by periphlebitis and vascular occlusion that progresses to retinal neovascularization with vitreous hemorrhage and tractional retinal detachment. Eales’ disease is considered idiopathic though many reports have theorized an association with Mycobacterium tuberculosis. The treatment is stage-dependent and may consist of oral corticosteroids, anti-VEGF injection, panretinal photocoagulation or surgery.
A: hypertensive retinopathy C: Mac Tel type 2
D: Coat’s disease
|
WHY BECOME AN ORS FELLOW?
By Bill Denton, O.D., F.A.A.O.
Chair, Membership Committee
At some point in your career, you realize you just may be coasting. Your knowledge has been limited to the journals you receive and attempt to read, and the conferences that may not be as fulfilling as they once were. You simply need a challenge that will add an extra dimension to your professional learning.
Fellowship in the Optometric Retina Society (ORS) can provide several benefits in addition to the initial challenge of qualifying for this honor. Plenty of perks accompany your induction, but the coolest part is being associated with a body of knowledge and resources which can help you in many other ways. It is not uncommon to receive weekly thought-provoking emails about challenging cases and treatment dilemmas. Some fellows like to share their awesome cases they have diagnosed, while others post their cases with hopes that other Fellows will suggest an alternative differential diagnosis. At times it is like a round-table of brainstorming, but through the use of modern technology. Fellowship has little obligation with a huge opportunity for professional growth.
If you are up to the challenge of becoming a Fellow of the ORS, feel free to peruse the details and application at www.optometricretinasociety.org. Advice can be given to assist you in your quest. Feel free to contact us.
|
Editor
in Chief
Anna K. Bedwell, OD, FAAO
Co-Editor
Brad Sutton, OD, FAAO |
Journal
Reviewers
Jenna Wellen, OD
Brooke Tobias, OD
Senior Graphic Designer
Matt Egger
|
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 11 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|