| |
|
| Vol. 2, #24 • Friday, October 15, 2021 |
|
|
|
|
| |
|
Review's Chief Clinical Editor
Paul M. Karpecki, OD, FAAO
Provides you with cutting-edge clinical strategies for optimal management of ocular surface disease and beyond.
|
|
|
|
|
|
It’s important to learn the two sub-types of dry eye, as each is treated quite differently.
According to TFOS DEWS II, there are two sub-types of dry eye: evaporative (EDE) and aqueous deficient (ADDE). Knowing how to treat each type is critical to successful outcomes, as the only overlapping features are inflammation and dry eye flares.
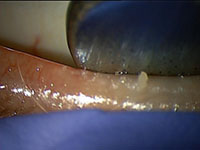
Evaporative Dry Eye
EDE, also known as lipid deficiency, involves meibomian gland dysfunction (MGD). It has unique components such as obstructed meibomian glands (MGs), blepharitis (Demodex or Staphylococcal), inflammation and an altered tear film.
 |
| EDE requires treating the obstructed meibomian glands and inflammation. |
For example, a case of mild EDE might be managed with a hydrating compress (obstruction), lid scrubs (blepharitis), omega fatty acids (inflammation), and a lipid-based artificial tear (tear film). A severe form of EDE, such as that associated with rosacea, might require in-office treatments like IPL/thermal pulsation or blepharoexfoliation, in addition to topical corticosteroids, neurostimulation, Lumify (Bausch + Lomb), and/or osmolarity-lowering tears.
Aqueous Deficient Dry Eye
In the case of ADDE, consider the two main components: inflammation and tear volume. Treatment might involve corticosteroids initially, followed by immunomodulatory agents like cyclosporine or lifitegrast, as well as osmolarity-lowering artificial tears, punctal occlusion, or even biologic agents. Biologic agents include amniotic membrane, cytokine extract drops, and autologous serum.
The Role of Inflammation
Hyperosmolarity induces inflammation, and all forms of dry eye disease are defined by hyperosmolar tears. Likewise, all forms of dry eye disease are associated with dry eye flares, given the nature of adaptive immunity associated with it. For that reason, ensure you control inflammation and flares, and in EDE, also treat the obstructed glands and any biofilm/blepharitis, which can lead to further inflammation. In ADDE, also elevate the tear volume via lubricants, punctal occlusion, and biologics such as serum tears.
|
|
|
|
KEY TAKEAWAY: For the sub-types of dry eye disease, be sure to treat the associated inflammation and dry eye flares along with other components that can include obstructed MGs, blepharitis, and the tear film.
|
|
|
|
| Supported by an independent medical grant from Kala Pharmaceuticals |
|
| |
| |
Review of Optometry® is published by the Review Group, a Division of Jobson Medical Information LLC (JMI), 19 Campus Boulevard, Newtown Square, PA 19073.
To subscribe to other JMI newsletters or to manage your subscription, click here.
To change your email address, reply to this email. Write "change of address" in the subject line. Make sure to provide us with your old and new address.
To ensure delivery, please be sure to add revoptom@lists.jobsonmail.com to your address book or safe senders list.
Click here if you do not want to receive future emails from Review of Optometry. |
|
|
|
|
|
|
|
|


