 |
|
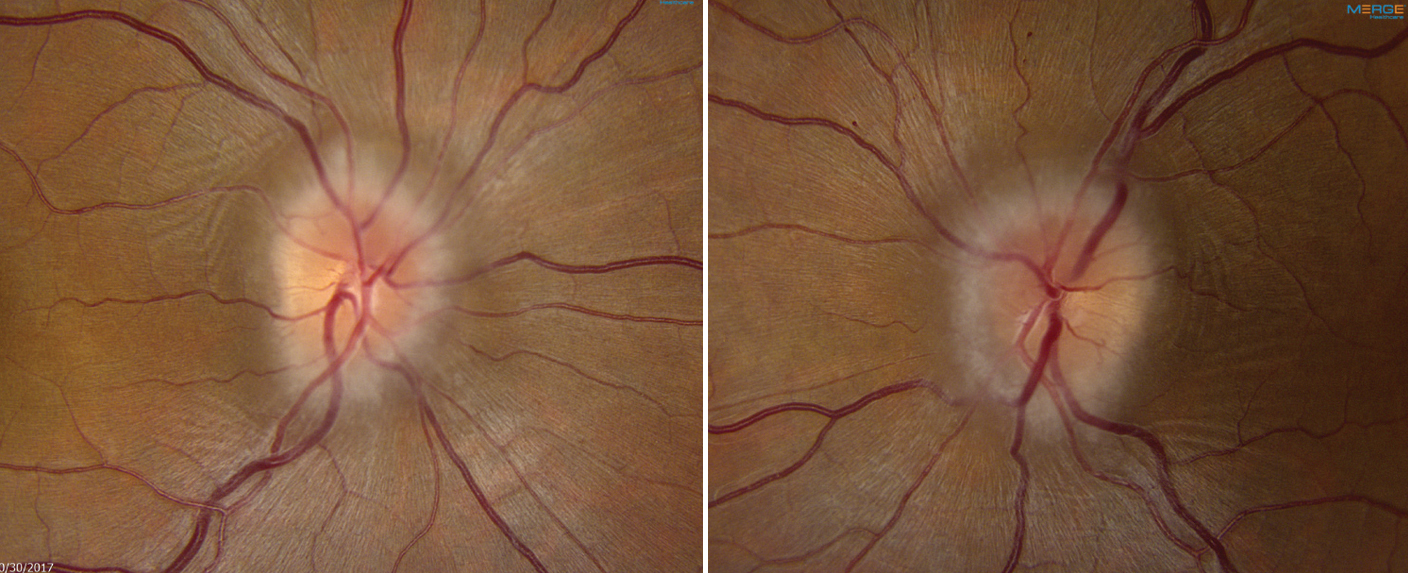
Patients with pseudopapilledema or known mild IIH, as well as patients with isolated radiologic signs of raised intracranial pressure, would have been more appropriately assessed in the outpatient setting than in the ED. Photo: Mark Dunbar, OD. Click image to enlarge. |
Once a relatively rare basis for consultation with a hospital emergency department or specialty practice, concern over suspected papilledema has grown in recent years. Many different factors are responsible for this ongoing change, including greater incidence of idiopathic intracranial hypertension (IIH), overreported radiologic signs of intracranial hypertension, strained access to outpatient neuro-ophthalmology services, poor insurance coverage and medicolegal concerns. These are all contributors to the lower threshold for emergency department (ED) visits for papilledema.
Consequently, one group of researchers wanted to examine the referral patterns and outcomes of neuro-ophthalmology ED and inpatient consultations for cases of concern for papilledema. Over one year, 153 consecutive patients were referred for concern of papilledema to a university-based subspecialty care center (Emory University) and underwent the institution’s standardized “papilledema protocol.”
After completing the protocol, it was determined that 58% of cases had bilateral optic disc edema, with 89% of those showing signs of papilledema (IIH). Of the 25% of the total consultations for suspected intracranial pressure without previous fundus exam, 74% did not have optic disc edema, 21% had papilledema and 5% had other causes of bilateral disc edema.
Of the 58% of consultations for presumed papilledema seen on fundus examination, 58% had confirmed papilledema, 17% had pseudopapilledema and 9% had other causes of bilateral optic disc edema. Of the 17% of patients with known IIH, five had papilledema and four required urgent intervention. Most diagnosed was IIH. Patients with secondary causes of IIH were on average older, men, not obese and more likely to have neurologic symptoms compared with IIH.
In total, the most common cause of bilateral disc edema was nonfulminant IIH in 64% of all referred patients without a previous diagnosis. The other 36% were diagnosed with a vision- or life-threatening disease, with 18 patients having papilledema from severe neurologic disorders.
In their paper for Journal of Neuro-ophthalmology, the study authors note that “it is impossible to predict which papilledema patients will have a potentially severe cause of raised intracranial pressure without urgent brain imaging, and even in cases of newly diagnosed IIH, predicting which patients will have a poor visual outcome and require urgent multidisciplinary treatment is challenging, highlighting the need for urgent evaluation.”
Further validating this urgency is the fact that seven urgent surgical interventions were performed in this IIH cohort to prevent vision loss, including two optic nerve sheath fenestrations, two primary cerebrospinal fluid shunting procedures and three shunt revisions.
The authors continue, pointing out that, “given the limited access to neuro-ophthalmologists, our study supports the need for ED access to expert eyecare providers or ocular fundus camera with remote interpretation of images for prompt identification of optic disc edema and standardized evaluation for neurologic emergencies such as with a ‘papilledema protocol.’”
Finally, they speculate that in the future, “implementation of nonmydriatic ocular fundus cameras and potential future artificial intelligence assisted triage and autonomous diagnosis of papilledema in the ED should allow expedited workup in unspecialized healthcare facilities.”
Ray HJ, Smolar ALO, Dattilo M, et al. The increasing burden of emergency department and inpatient consultations for ‘papilledema’. J Neuroophthalmol. March 19, 2024. [Epub ahead of print]. |