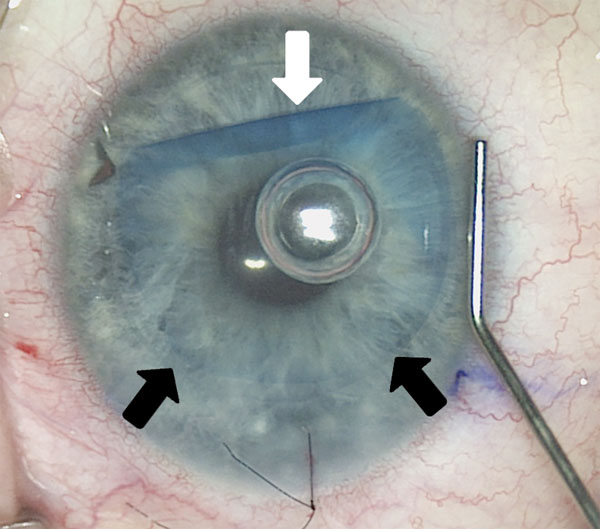
Closed Off
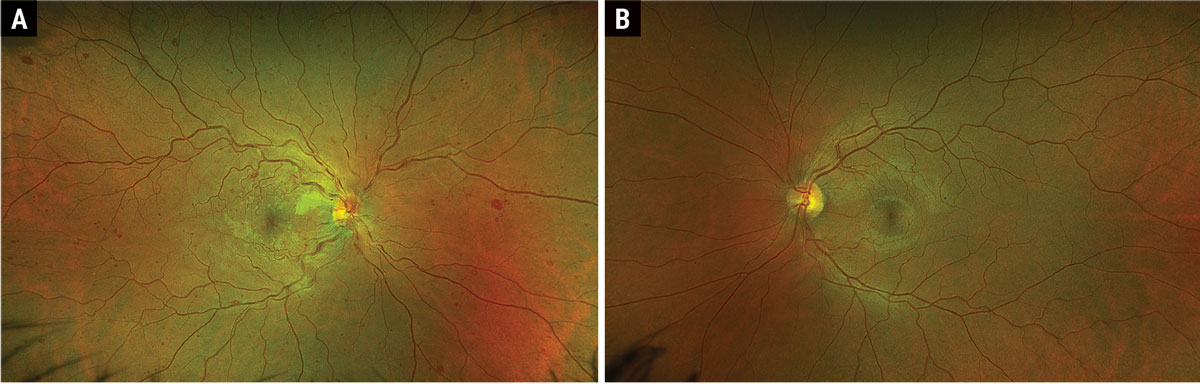
A 35-year-old Hispanic male presented with acute onset painless “cloudy vision” OD for four days. The patient recalled a similar event of transient monocular vision loss OD four months prior that was self-limiting within three hours that he never sought medical care for.
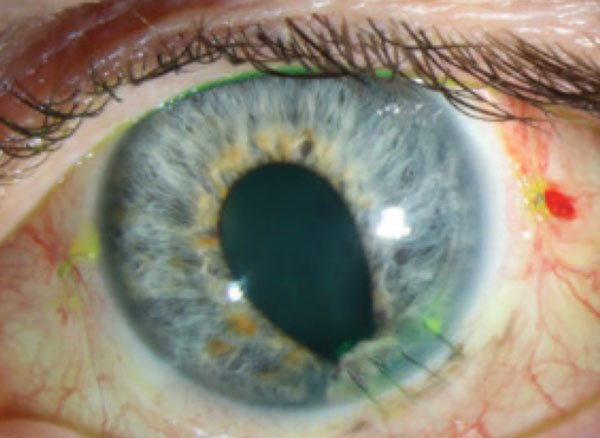
Don’t Chicken Out with These Pox
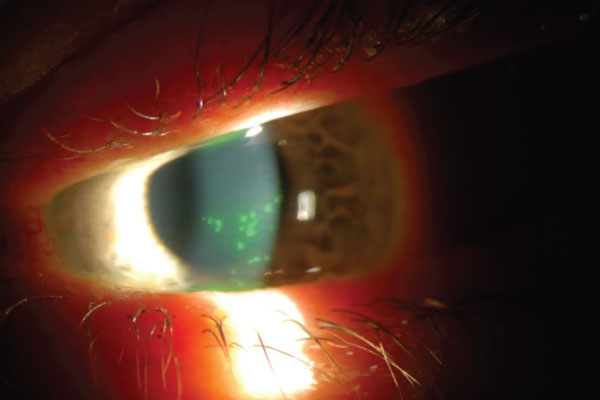
A 63-year-old male presented to the emergency room (ER) for onset of pain experienced two days prior, starting with left ear pain that radiated over to the left temporal side of his face, including his jaw. He reported “the muscles in his eye hurt” and had pain on eye movement. He also reported his eyeball was “irritated” and had tearing.
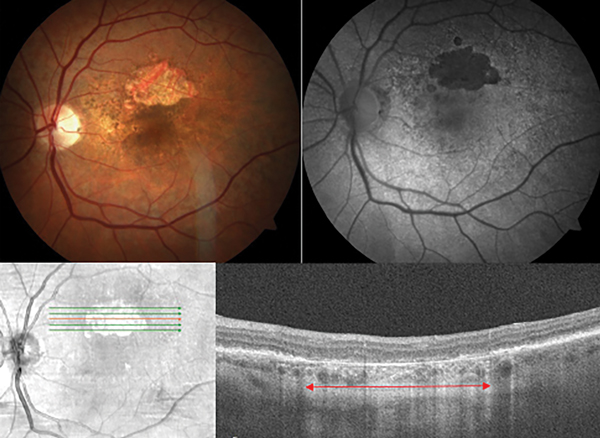
Enough Data to Track Glaucoma Patients?
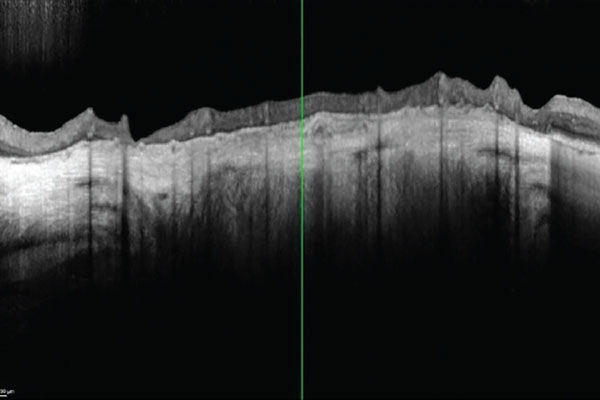
When you’ve been in practice for many years and the number and variety of glaucoma scenarios you’ve encountered is rather large, you learn to manage these patients the best you can with the information that is available to you. For example, some patients physically are unable to perform visual field testing and OCT imaging; some cannot be examined with a slit lamp. Still others have media opacification that prohibits adequate visualization of the posterior pole. So, how do you handle them? This recent scenario is a perfect example of maximizing use of our technology to gather as much information as is possible.
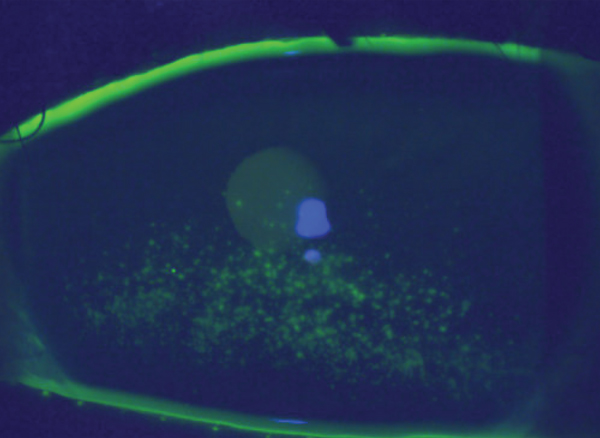
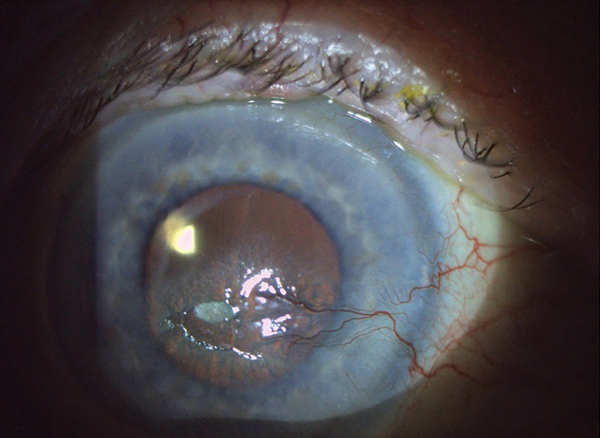
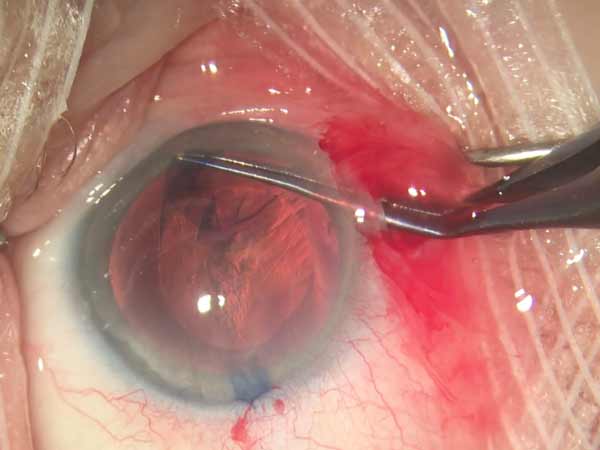
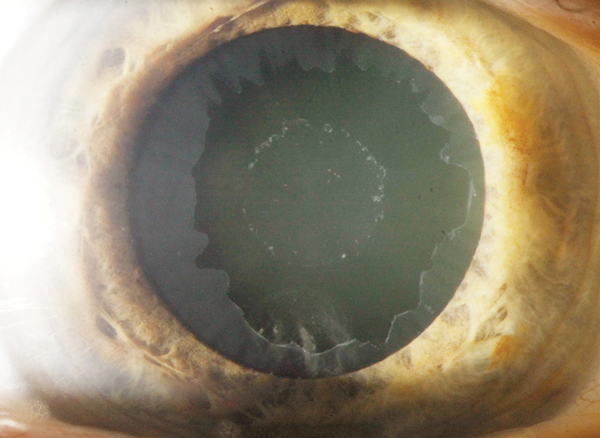
Double-edged Sword
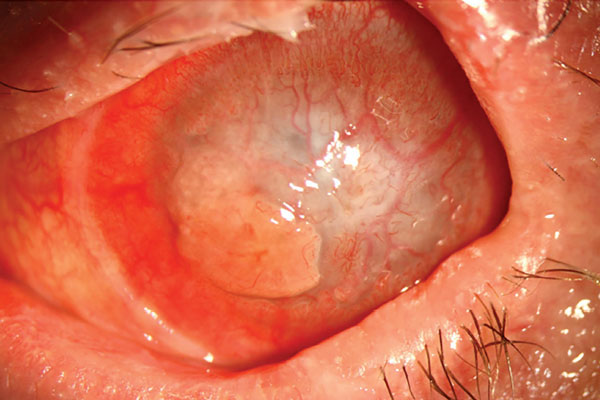
A 30-year-old patient presented to the contact lens (CL) clinic with a history of Stevens-Johnson syndrome (SJS). His chief complaints included chronic pain, blurry vision and dryness of the left eye.
Twin Tumor Therapies
Tivdak and Elahere are important advances for disease control in aggressive, often difficult-to-treat gynecological cancers.
The News Feed
Handheld AI Fundus Camera Detects DR in 60 Seconds
Ganglion Cell Complex Thickness Reduced in AMD
Meds that Induce Angle-Closure Glaucoma Identified
Uveitis Recurrence Risk Elevated After COVID-19 Vaccination
Nutraceutical for Dry Eye Coming This Fall
Vision-related QoL Unchanged After Trabeculectomy
Smoking Reduces ONH Vessel Density in Glaucoma
AREDS Report Updates Simplified Severity Scale
Study Finds Prophylactic LPI Cost-Effective for PACS
Red Light Therapy Less Effective in Pre-myopia Phase
MEWDS Characterized by Unique Photoreceptor Damage Patterns
Lamina Cribrosa Pores May Help Identify Severe Glaucoma
Optic Nerve Head Structure Affected by Birth Status
Patient Survey Describes Dry Eye Management Habits, Burdens
Study: Epi-off Accelerated CXL Yields Good Results
Heavy Smoking, High BMI Associated With Earlier Onset nAMD
Access to Pediatric Eye Care Severely Lacking Across the US

Look Inside The Current Issue
Features
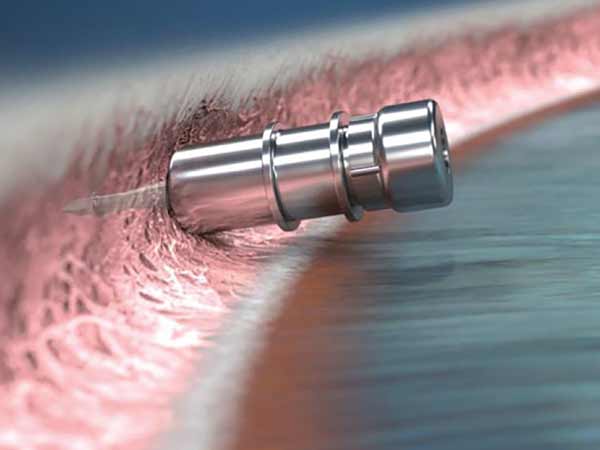
Advances in Endothelial Surgery: An Update for ODs
Corneal Cases: Which are Right For You?

Building a Top-Flight Staff
Corneal Pain Presentations: Causes and Interventions
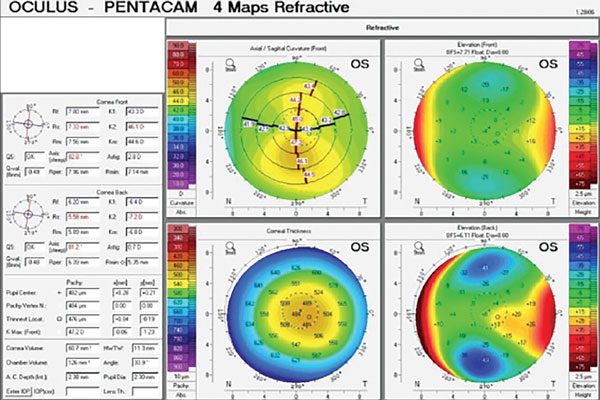
Sizing Up Keratoconus: The Roles of Topography and Tomography
Departments

Attack of the Clones
Big Things in Small Packages
Corneal and Allergy Conundrums
Enough Data to Track Glaucoma Patients?
Flashes? Think Beyond the Retina
Hot Topic

The Enemy Within
Twin Tumor Therapies

Upcoming Events


Continuing Education
Corneal Pain Presentations: Causes and Interventions
OCT Beyond the Basics: Unlocking the Power of This Essential Tool
Demystifying the Complement System
The Physical Manifestations of Glaucoma and What They Signify
Additional Publications
-
The Value of Real Tears
Francis Mah, MD, and Jessica Steen, OD, FAAO, discuss the importance of a stable tear film, how real tears help maintain the health of the ocular surface and the effect that various dry eye interventions can have on tear film homeostasis.
Sponsored by Viatris A Wider View Of The Retina Advances Care
It’s Time to Talk to Your Patients about Digital Eye Strain
New Developments in Glaucoma
Ophthalmic Product Guide - February 2024
Preservatives in Eye Care: Intrepid Eye Society Consensus Discussion
Review of Cornea & Contact Lenses
-
Custom vs. Standard Soft Lenses for the Irregular Cornea: How to Choose
Learn which approach works best in this case-based article. -
Corneal Topography: Get to New Heights
See how elevation data reveals the greatest truths about corneo-scleral shape. -
Soft Toric Lenses: Harness This Valuable Practice Opportunity
Experts demystify common misconceptions and offer fitting pearls. -
Wave Hello to Wavefront-Guided Sclerals
These lenses are a great option for those with residual higher-order aberrations but also can be used to create excellent multifocals. -
GP Multifocal Contact Lenses: The 2024 Lineup
Recent design advancements give clinicians even more options to help meet patients’ vision demands. -
Empirical Fitting of GP Lenses
Advanced technology has paved the way for a quite easy and successful approach.
Women In Optometry continues to be published online, with regular updates on practice design, practice success, news, trends and perspectives. Visit womeninoptometry.com.
Job of the Week
