 |
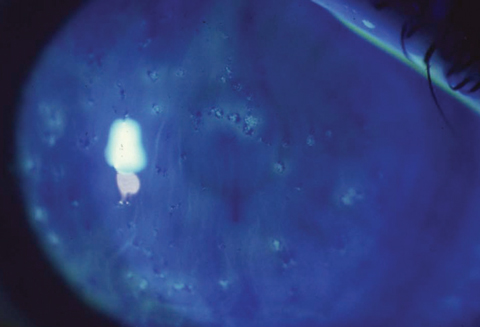
Clinicians shouldn’t be too quick to rule out stromal involvement in Thygeson’s superficial punctate keratitis. Though it’s true that the epithelium is the structure primarily affected, stromal inflammation and scarring can also accompany it. Photo: Ron Melton, OD, and Randall Thomas, OD. Click image to enlarge. |
A recent editorial in the Ophthalmology journal addressed six habits of thought and/or practice that, once entrenched, can hold back effective care of various anterior segment conditions.
The first myth noted by the authors is that of believing that Hutchinson’s sign is uniquely predictive of herpes zoster ophthalmicus. The authors point out that John Hutchinson himself never stated nose tip involvement indicated a higher risk of ocular involvement in zoster of the first dermatome of the fifth cranial nerve.
In fact, larger studies indicate any rash in the nasociliary dermatome (and not just the tip of the nose) possesses at least some predictive value for ocular involvement as well. However, with common false-negative and false-positive findings, this raises questions about how useful Hutchinson’s sign is diagnostically. The authors instead believe all V1 zoster patients should be evaluated for ocular involvement, supported by another study that found V1 zoster patients in the emergency department did not have predictive ocular involvement upon Hutchinson’s sign.
The second myth addressed the common practice of advocating baby shampoo lid scrubs as a first-line treatment for blepharitis. The authors first point to a 2012 Cochrane review concluding no strong evidence exists for any treatment of chronic blepharitis. They also point out that the primary ingredient in Johnson & Johnson’s baby shampoo, cocamidopropyl betaine, was the 2004 Contact Allergen of the Year as determined by the American Journal of Contact Dermatitis, and in fact has the potential to destabilize the tear film and injure the ocular surface.
Myth three concerns Thygeson’s superficial punctate keratitis (SPK). Philips Thygeson noted that only the corneal epithelium was involved in SPK and never scarred. However, since his manuscript was published in 1950, multiple authors have since described cases of SPK with anterior stromal inflammation, corneal scarring or both.
Number four clarifies that superior limbic keratoconjunctivitis (SLK) is not in fact caused by tight upper eyelids. SLK is associated with thyroid eye disease and graft vs. host disease (GVHD), and for patients with thyroid eye disease, only a small percentage of these cases demonstrate SLK, with none measuring tighter lids compared with controls. GVHD patients with SLK demonstrate greater eyelid laxity, not less, than controls.
Nonpreserved artificial tears have been recommended for prescription for patients using them frequently, mostly out of deference to protecting the ocular surface from exposure to harmful preservatives. Myth five tackles just that, with the authors stating that little to no data points toward therapeutic superiority of nonpreserved options. Instead, they believe nonpreserved artificial drops should be used if ocular irritation occurs from a preserved version.
The last point discussed is the conventional wisdom that topical corticosteroids need to be tapered to avoid rebound inflammation. Two problems exist with this thinking, the authors say. First, they found no data supporting the notion that the eye becomes steroid-dependent as soon as ocular steroids are administered. Second, the word “rebound” suggests in this context that recurrent inflammation is occurring when steroids are reduced, rather than that the actual unresolved inflammatory process will recur once therapy is stopped.
The authors explain that with these examples, there is an acknowledgement of misinformation lingering in the field. Going forward, they conclude, “our educators and trainees constantly need to develop a culture and curriculum of critical thinking and skepticism.”
Margolis TP, Galor A. Six myths of the anterior segment: misunderstandings and critical thinking in ophthalmology. Ophthalmol. March 30, 2023. [Epub ahead of print]. |