 |
Results from the BLINK Study suggest that treatment effect for myopia control is similar for all rates of progression in children and that soft multifocal contact lenses don’t affect comfort, focus or how well the two eyes work together. Photo: CooperVision. Click image to enlarge. |
Two presentations given at ARVO New Orleans evaluated reports from the BLINK (Bifocal Lenses in Nearsighted Kids) Study on multifocal contact lens myopia control. The first one compared myopia progression and axial elongation in children wearing +2.50D add multifocal vs. single-vision contact lenses to find out whether the treatment effect of optical myopia control is better for fast progressors, and results suggest that children receive a similar amount of treatment benefit from myopia control regardless of their underlying rate of progression.1
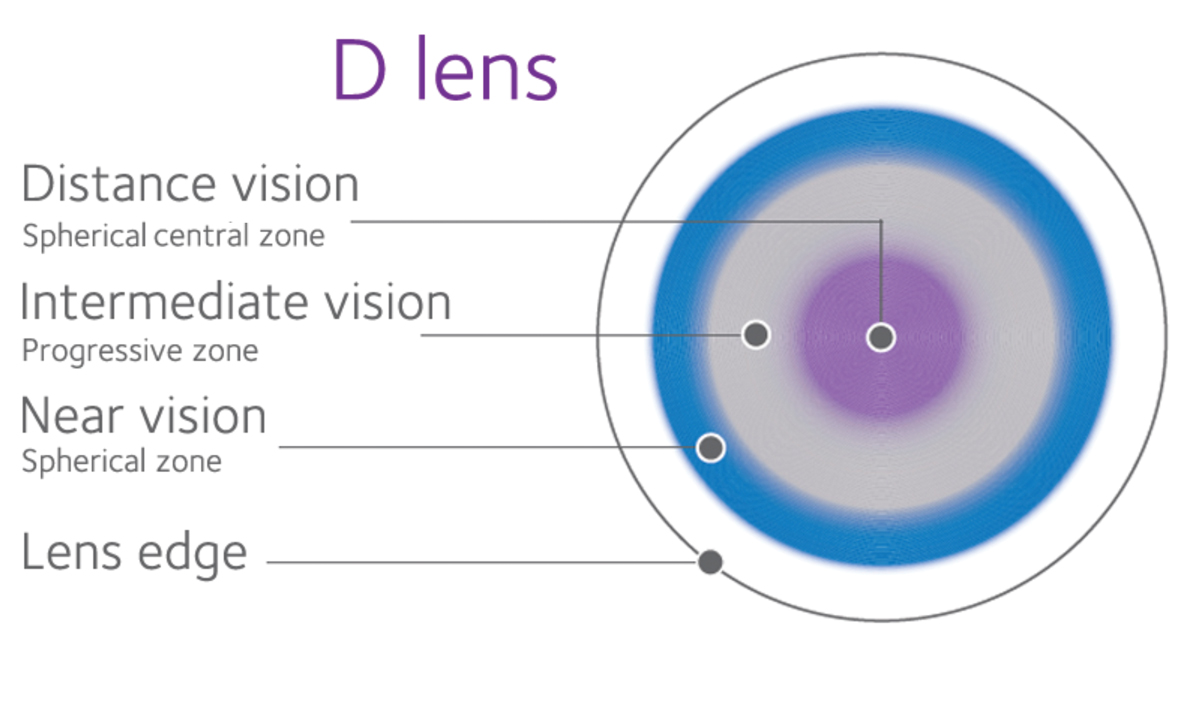
The BLINK Study randomized 294 children between the ages of seven and 11 to wear Biofinity soft contact lenses for three years in either a D-design with a +2.50D add, +1.50D add (not analyzed in this study) or single-vision contact lenses. Cycloplegic refractive error was between -0.75D to -5.00D (sphere, inclusive) at baseline with less than 1.00D of astigmatism. Three-year myopia progression and axial elongation for single vision (n=96) and +2.50D add (n=95) groups were plotted against their cumulative frequency Z-scores with slopes estimated by linear regression.
Differences between treated and control groups only varied by ±0.11D across two standard deviations of myopia progression with no significant variation across the range of axial elongation. The variations were not large enough to create meaningful differences between the treated and control groups over three years. “A uniform treatment benefit suggests that all children should be considered candidates for optical myopia control rather than prioritizing those at risk for fast progression,” the authors concluded in their abstract.
The second presentation compared Convergence Insufficiency Symptom Survey findings, phoria and accommodative lag between single-vision and multifocal contact lens wearers with 1.50D add and +2.50D add over three years and found that myopia control with soft multifocal contact lenses does not negatively affect how well the two eyes work together, how accurately they focus on a near target or the comfort of the eyes.2
The accommodative lag was less than baseline at all visits for the three groups, except the lag was similar between baseline and two weeks for +2.50D add. The only differences observed were between single vision and +2.50D add at two weeks and one year and between single vision and +1.50D at two weeks. The maximum difference between groups in average accommodative lag was never more than 0.33D. Near phoria was statistically significantly more exophoric after baseline for both add powers but never became more than 2.40 prism diopters more exophoric over the three years. The +2.50D add group was more exophoric than the single-vision group at all visits after baseline but never more than 2.00 prism diopters more exophoric on average over three years.
Original abstract content © Association for Research in Vision and Ophthalmology 2023.
1. Mutti DO, Sinnott LT, Berntsen DA, et al. Uniformity of treatment benefit in multifocal contact lens myopia control. ARVO 2023 annual meeting. 2. Walline JJ, Tomiyama E, Sinnott LT, et al. Phoria, accommodative lag and symptoms of soft multifocal contact lens myopia control. ARVO 2023 annual meeting. |