 |
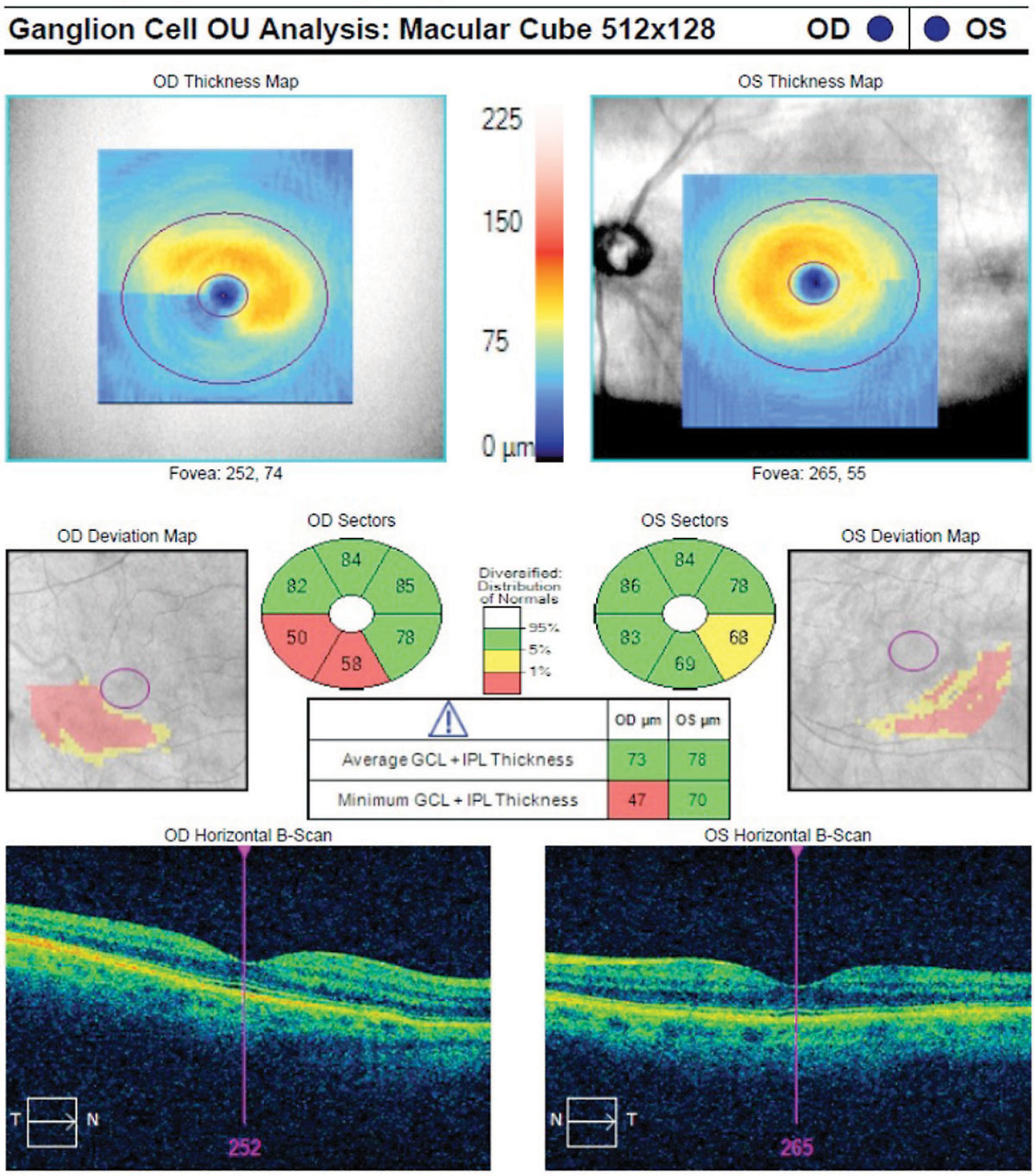
| Diagnosis of glaucoma in highly myopic eyes can be difficult, with certain OCT parameters trumping others. Macular ganglion cell-inner plexiform layer proved decisive in this study. Photo: Danica Marrelli, OD. Click image to enlarge. |
The diagnosis of glaucoma in highly myopic eyes can be challenging, as the patient’s ocular anatomy often mimics that of someone experiencing glaucomatous changes. A recent study compared the glaucoma detection utility of various OCT parameters for high myopia, concluding that certain factors may play a more significant role than others.
The retrospective cross-sectional study was conducted for eight years.1 A total of 132 participants with high myopia (axial length 26mm or spherical equivalent -6D) plus glaucoma and 142 participants with high myopia without glaucoma were recruited. Macular ganglion cell-inner plexiform layer (GCIPL) thickness, peripapillary retinal nerve fiber layer (RNFL) thickness and optic nerve head (ONH) parameters were measured in each participant.
The area under the curve (AUC) —a statistical measure of the correspondence between variables—for a set of glaucoma prediction criteria called the University of North Carolina OCT Index was 0.891, and the AUC of temporal raphe sign positivity was 0.922. The best single OCT parameter was inferotemporal GCIPL thickness, with an AUC of 0.951; it differed from the UNC OCT Index, temporal raphe sign, mean RNFL thickness and ONH rim area by 0.060, 0.029, 0.022 and 0.075, respectively.
The researchers concluded that, in discriminating glaucomatous eyes in patients with high myopia, inferotemporal GCIPL thickness yielded the highest AUC value. “The RNFL thickness and GCIPL thickness parameters may play a greater role in glaucoma diagnosis than the ONH parameters in high myopia.”
A commentary also published in JAMA Ophthalmology in response to this study and others highlighted the importance of the findings due to the “diagnostic dilemma” patients with high myopia pose to clinicians.2 The authors noted that detecting coexisting glaucoma in this specific cohort can be challenging because the characteristically small ONHs make it difficult to appreciate signs of glaucomatous damage. Such findings in these patients may also masquerade as glaucoma, complicating diagnosis and treatment, the commentary noted.
Based on the findings of the study mentioned earlier and others, the commentary authors concluded, “Careful review of the OCT B-scan to identify artifacts and correct tracing errors, as well as use of the macular thickness map to confirm asymmetric arcuate losses, will continue to be critical when deciding whether glaucomatous damage is present in eyes with high myopia.”
1. Jeong Y, Kim YK, Jeoung JW, Park KH. Comparison of optical coherence tomography structural parameters for diagnosis of glaucoma in high myopia. JAMA Ophthalmol. May 18, 2023. [Epub ahead of print]. 2. Asrani S, Thompson AC. Which optical coherence tomography parameter, if any, identifies glaucoma in high myopia? JAMA Ophthalmol. May 18, 2023. [Epub ahead of print]. |