 |
A 73-year-old Caucasian female was referred to me by a neuro-ophthalmic colleague for continued care. The patient had relocated to my area about 18 months prior, and she brought with her a lengthy history involving a pituitary adenoma that had been resected 10 years earlier. She had also undergone bilateral cataract surgery approximately six years earlier. Essentially, the patient had been stable prior to moving to the area and was continuing care with new providers. She had been seen most recently by neuro about three months prior to my first visit with her.
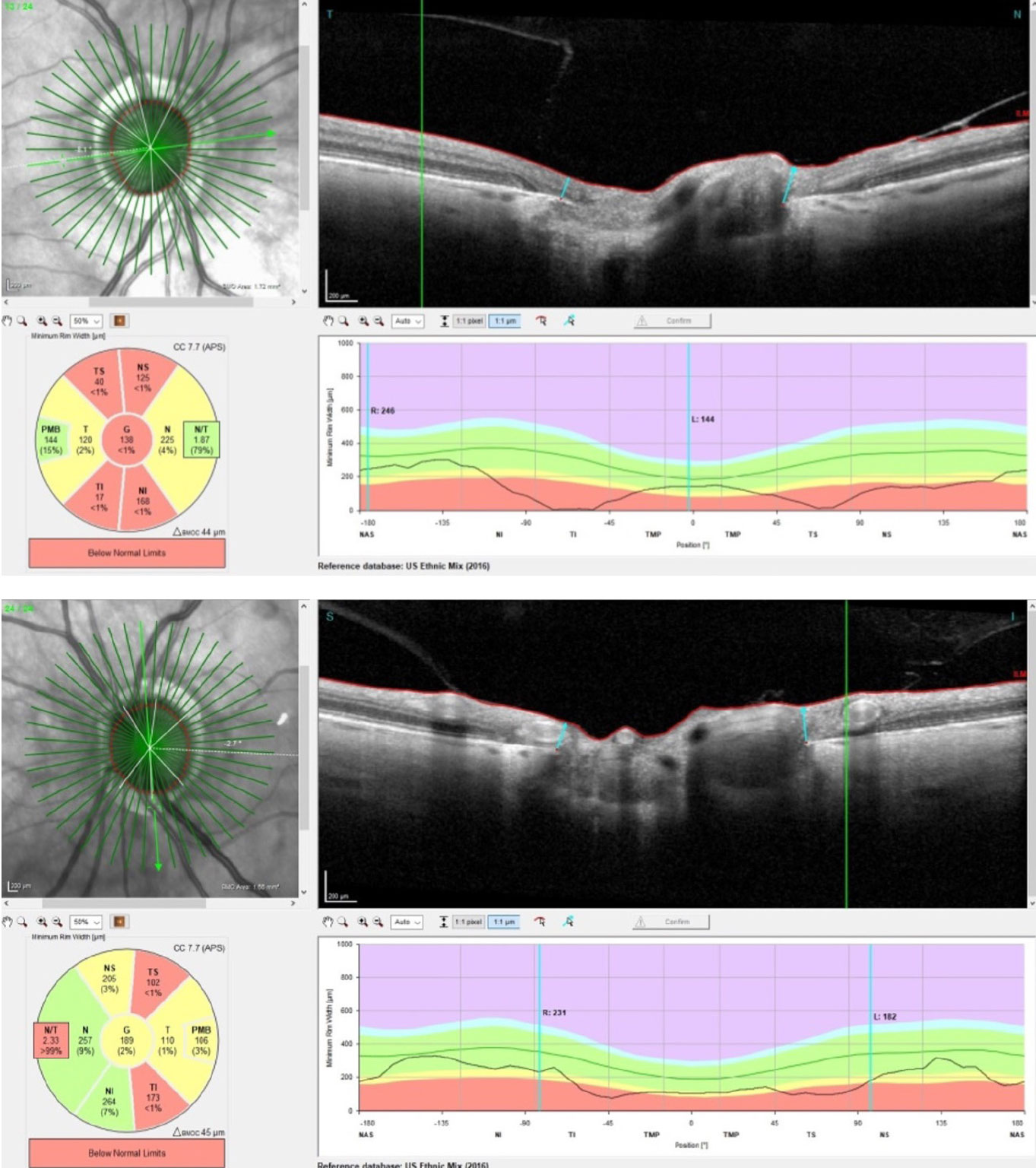 |
| The radial BMO-MRW scans of the patient’s right (top) and left (bottom) eyes. Note the OCT segmentation of the PMB in each eye; interestingly, the right PMB is essentially normal, and the left is somewhat compromised. Click image to enlarge. |
The Case
At the initial visit her entering visual acuities were 20/50- OD and 20/40- OS. She complained of some increased blur interfering with her daily activities. Best-corrected visual acuities through hyperopic astigmatic and presbyopic correction were 20/40+ OD and 20/40+ OD. Pupils were equal, round and reactive to light and accommodation, with no afferent pupillary defect. Extraocular muscles were full in all positions of gaze.
Slit lamp examination of her anterior segments was essentially unremarkable. There was mild epithelial basement membrane dystrophy present OU, the anterior chamber angles were open 360° and the chambers were quiet. There was mild dermatochalasis present bilaterally. Applanation tensions were 14mm Hg OD and OS.
Through dilated pupils, her posterior chamber intraocular lenses were clear and centered; the posterior capsules were opened secondary to YAG capsulotomies OU. Bilateral posterior vitreous detachments were present.
Close stereoscopic examination of her optic discs revealed some not so surprising findings and one remarkable finding. Both optic nerves were pale and of normal size. The pallor was subtle but distinctly present. There was some peripapillary atrophy present OU, making physical examination of the edges of the optic disc and cup somewhat difficult. She also had rather significant optic cupping; her cup-to-disc ratios were estimated to be 0.7 x 0.9 OD and 0.65 x 0.75 OS.
The presence of both the optic atrophy and loss of axons at the optic nerve is not surprising in patients with pituitary issues such as this one. She had initially presented to her primary care provider many years ago with headaches that prompted neuroimaging. The pituitary adenoma was found at that time, but there weren’t any significant ancillary issues that warranted surgical intervention at that time.
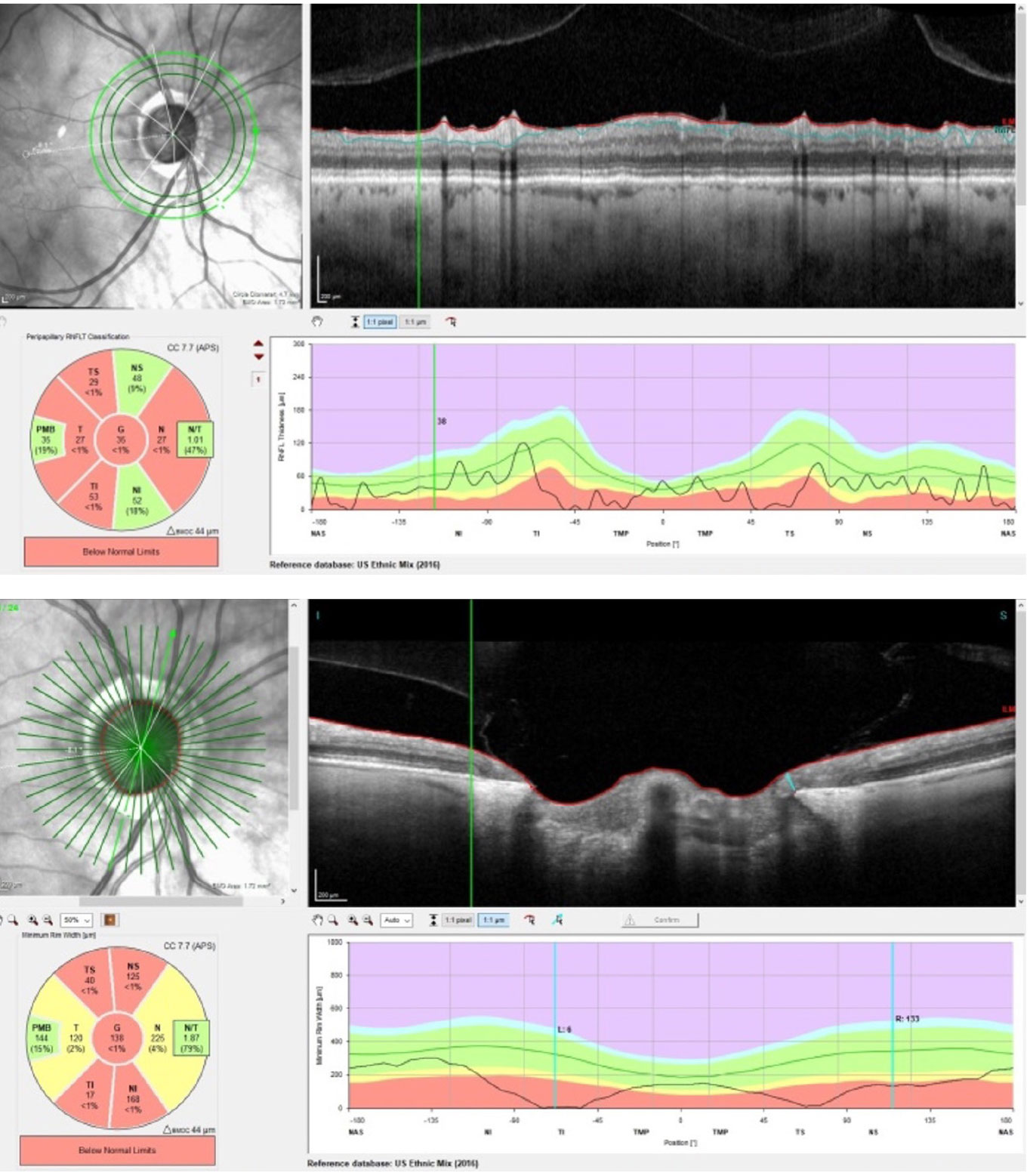 |
| Superior temporal and inferotemporal RNFL thinning OD, not inconsistent with glaucoma, with preservation of the PMB (top). An eroded inferotemporal neuroretinal rim with a paltry 6µm of tissue remaining at the scan marker (bottom). Click image to enlarge. |
Ultimately, after several years, symptoms increased and so did the adenoma, ultimately requiring surgical resection. Symptoms included changes in vision, headaches and involvement of the cavernous sinuses on both sides.
Following surgical intervention, her symptoms subsided. But given the protracted length of time the adenoma was present and gradually involving the chiasm, the atrophy and pallor were not surprising. What I did find surprising was the extent of her optic cupping bilaterally.
Her macular evaluations were characterized by retinal pigment epithelial granulation and drusen OU, consistent with her somewhat reduced acuity. There was no clinical evidence of neovascular age-related macular degeneration. The retinal vasculature was characterized by mild arteriolarsclerotic retinopathy and crossing changes. Her peripheral retinal evaluations were unremarkable.
Following the dilated fundus examination, I ordered a neuro profile OCT of her optic nerves. This particular optic nerve OCT segments out not only the circumpapillary retinal nerve fiber layer (RNFL) and Bruch’s membrane opening-minimum rim width (BMO-MRW) as do the standard glaucomatous optic nerve scans but also the papillomacular bundle (PMB) fibers. As you know, the PMB fibers head straight to the optic nerve from the ganglion cells adjacent to the fovea, and these fibers are often damaged in non-glaucomatous optic neuropathies and under inflammatory optic nerve conditions, such as optic neuritis.
My OCT protocol when there are neuro-ophthalmic findings that can affect the optic nerve is to run this type of scan, as it tells me what I need to know from a glaucoma perspective and also sheds light on any concurrent neuro-ophthalmic problems.
While these OCTs demonstrated sectorally thinned neuroretinal rims, what I found interesting was the preservation of the PMB in the right eye and somewhat compromised PMB in the left. Furthermore, the extent and characteristics of the optic disc neuroretinal rim loss were also suggestive of glaucomatous damage as seen in the inferotemporal and superior temporal segments of each nerve, more noticeable OD than OS. This can even be seen in the perioptic RNFL OD in the 4.7mm circle scan, somewhat distant from the neuroretinal rim.
Upon interpreting these OCT reports, I was concerned about the possibility, and frankly probability, of this patient also having concurrent normal-tension glaucomatous damage to both optic nerves (OD>OS).
I discussed the findings with the patient and asked to see her back in a week to run threshold fields and pachymetry.
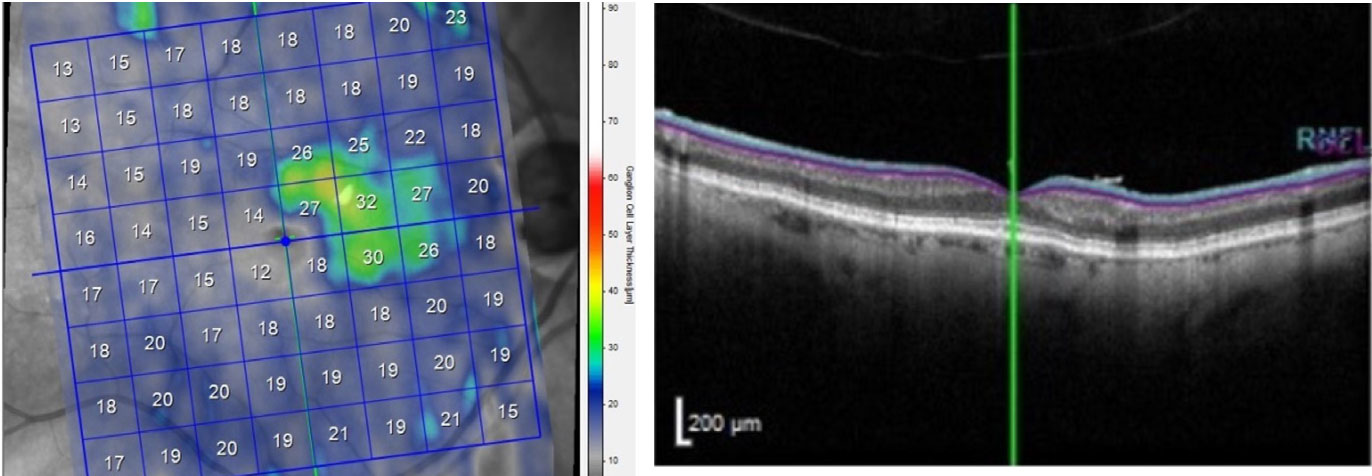 |
| Significant macular ganglion cell layer loss OD, except for the ganglion cells in the PMB. Click image to enlarge. |
The Outcome
The patient returned as requested. At this visit, applanation tensions were 15mm Hg OD and 14mm Hg OS. Pachymetry was 537µm OD and 540µm OS. Threshold visual fields demonstrated several things, namely bitemporal field loss OU, with the vertical meridian affected OS at fixation, as well as superimposed bilateral arcuate defects above and below OD>OS consistent with glaucomatous field loss. In essence, the field defects demonstrated bitemporal hemianopia consistent with the chiasmal/pituitary problem, more noticeable in the left eye, along with arcuate field defects consistent with glaucoma, more noticeable in the right eye.
The preservation of a portion of the macular ganglion cell layer in the right eye accounts for why the vertical meridional field defect OD did not involve fixation.
I discussed my findings with the patient and explained the concurrent presence of normal-tension glaucoma and the need to therapeutically intervene. Intraocular pressure (IOP)-lowering drops were prescribed, and at the follow-up about 12 days later, IOPs had been reduced to 9mm Hg OD and 10mm Hg OS. The medication was well-tolerated.
Later that day, I spoke with neuro, and after seeing the images, we agreed on the concurrent pressure-independent glaucomatous findings. The patient is scheduled to see me again next month for continued care.
Working closely with interdisciplinary colleagues, including other ODs, who appreciate your skills is satisfying professionally and ultimately makes better patient care possible.
Dr. Fanelli is in private practice in North Carolina and is the founder and director of the Cape Fear Eye Institute in Wilmington, NC. He is chairman of the EyeSki Optometric Conference and the CE in Italy/Europe Conference. He is an adjunct faculty member of PCO, Western U and UAB School of Optometry. He is on advisory boards for Heidelberg Engineering and Glaukos.
