 |  |
For some time, Descemet’s membrane endothelial keratoplasty (DMEK) has been the preferred procedure for treating Fuchs’ endothelial disease. However, Descemet stripping only (DSO)—also known as descemetorhexis without endothelial keratoplasty—may eliminate the need for DMEKs in patients with centrally isolated Fuchs’ corneal dystrophy.
Strip Away
This procedure is indicated in eyes with guttate within 5mm of the central cornea with a clear peripheral cornea and endothelial cell count of >1,000 cells/mm2 seen on specular or confocal microscopy. Contraindications for DSO include presence of Descemet’s membrane folds, any stromal pathology (e.g., bullae, stromal haze) presence of other corneal pathology, history of herpes keratitis and endothelial cell count below 1,000 cells/mm2.1 It is imperative that the peripheral cornea is clear and that guttate is isolated centrally in patients prior to DSO. Patients should also not have any stromal disease or history of keratitis.
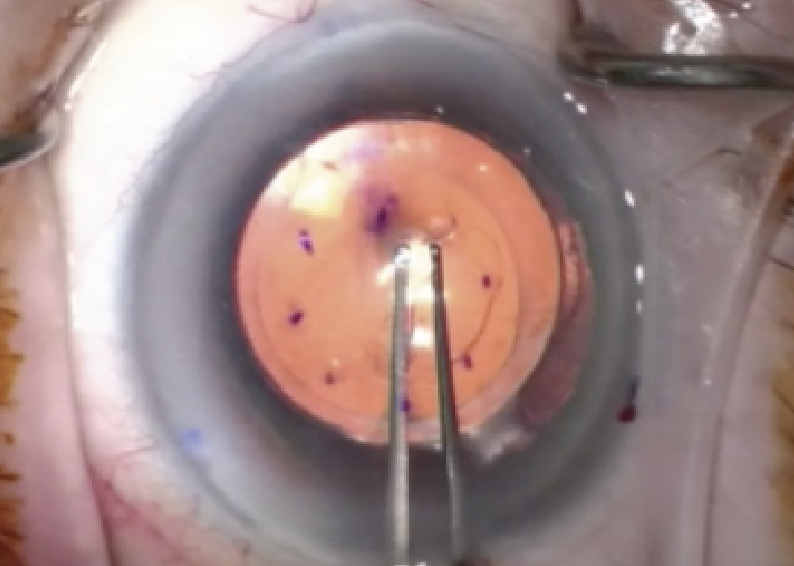 |
| Descemet stripping only allows a person’s own endothelial cells to redistribute, skipping the need for a cornea transplant. Click image to enlarge. |
DSO can be performed in both phakic and pseudophakic eyes and is relatively quick, performed in approximately five to six minutes under local anesthesia; it does not require injection of air or gas into the anterior chamber.2
Surgeons may choose to dilate the pupil beforehand to obtain a better red reflex and therefore better visualization of Descemet’s. Using viscoelastic, a central circular descemetorhexis of approximately 4mm to 5mm is performed using a Sinskey or Fogla Descemet’s membrane stripping hook. It is important that Descemet’s is carefully peeled and not scraped, as scraping can cause a larger descemetorhexis, as well as involvement of the stroma.
During the healing process, peripheral endothelial cells from the healthy cornea migrate toward the central area of the descemetorhexis and regenerate the central posterior cornea.
Postoperative treatment should include topical steroids, antibiotics and hypertonic sodium chloride. It has also been shown that rho-kinase inhibitors can increase endothelial cell proliferation, suggesting that its post-op use can decrease corneal edema and increase corneal clarity.3,4
Advantages and Complications
A great advantage of DSO is the elimination of donor tissue implanted in the eye. This alone prevents some of the postoperative complications involved in DMEKs such as graft rejection, potential IOP spikes from gas in the anterior chamber that’s used to initially hold the graft in place and the risk for secondary procedures such as a refloat. DSO also eliminates the need to perform a prior peripheral iridotomy and supine positioning following surgery. However, like any procedure, DSO also has potential complications, including decentration of the descemetorhexis that can impede visual acuity or cause posterior stromal opacity, irregular corneal astigmatism, persistent corneal edema and Descemet’s membrane detachment.
Although there is a longer healing period compared to DMEK, DSO has shown similar visual outcomes with fewer adverse events.1,5
Dr. Cunningham is the director of optometry at Dell Laser Consultants in Austin, TX. He has no financial interests to disclose. Dr. Whitley is the director of professional relations and residency program supervisor at Virginia Eye Consultants in Norfolk, VA. He is a consultant for Alcon.
Dr. Panda completed her residency in ocular disease and ocular/refractive surgery management at Virginia Eye Consultants in Norfolk, VA, where she currently works as a provider. She has no financial disclosures.
1. Moloney G, Petsoglou C, Ball M, et al. Descemetorhexis without grafting for fuchs endothelial dystrophy-supplementation with topical ripasudil. Cornea. 2017;36(6):642-8. 2. Ploysangam P, Patel SP. A case report illustrating the postoperative course of descemetorhexis without endothelial keratoplasty with topical netarsudil therapy. Case Rep Ophthalmol Med. 2019;6139026. 3. Okumura N, Kinoshita S, Koizumi N. Application of rho-kinase inhibitors for the treatment of corneal endothelial diseases. J Ophthalmol. 2017;2646904. 4. Ploysangam P, Patel SP. A case report illustrating the postoperative course of descemetorhexis without endothelial keratoplasty with topical netarsudil therapy. Case Rep Ophthalmol Med. 2019;6139026. 5. Hamzaoglu EC, Straiko MD, Mayko ZM, et al. The first 100 eyes of standardized descemet stripping automated endothelial keratoplasty versus standardized Descemet membrane endothelial keratoplasty. Ophthalmology. 2015;122(11):2193-9. |
