 |
A 27-year-old Caucasian female patient reported to the office with a chief complaint of dry, irritated eyes of two weeks’ duration. She explained that her eyes became red over the previous two weeks and that use of Visine made them less red but didn’t stop the discomfort.
The patient’s systemic and ocular histories were unremarkable and she denied exposure to chemicals or allergies of any kind. However, she had recently started oral over-the-counter allergy medications for the symptoms of clogged ears.
 |
|
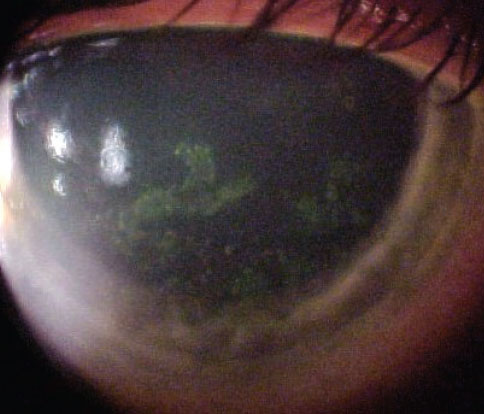
Slit lamp exam of the patient revealed these findings. What might be the origin? Click image to enlarge. |
Her best-corrected entering visual acuities were 20/20 OU at distance and near. External examination was normal with no evidence of afferent pupillary defect. The biomicroscopic examination of the anterior segment is demonstrated in the photograph. Goldmann applanation tonometry measured 15mm Hg OU. The dilated fundus findings were normal peripherally and centrally, with normal nerves and maculae.
Additional studies included examination of the eyelids for blepharitis, distichiasis or trichiasis. The phenylephrine blanch test could also be employed to assess the depth of the inflammation. Sodium fluorescein staining was completed to assess the status of the corneal epithelium. The lacrimal lake should be observed and Schirmer tear testing can be completed to quantify the volume of tear production.
Diagnosis
The condition discussed in this issue is dry eye perpetuated by the initiation of oral antihistamines. Medical interventions necessitate management of the underlying cause. There are four principle etiologies that contribute to ocular surface disease: (1) mechanical issues, (2) lipid dysfunction, (3) aqueous deficiency and (4) mucus deficiency.1-7
Ocular surface anatomy includes tear production apparatus (lacrimal gland, glands of Wolfring and Krauss), the lipid glands preventing evaporation (meibomian, Zeiss and Moll) and adnexa contributing to lid-globe congruity and tear movement (conjunctivae, pars ciliaris, pars lacrimalis, and nasal lacrimal system).1-7 Interruption here creates surface dryness and accompanying symptoms.1-11
Mechanical issues can be divided into three subcategories:12-21
(1) medical/environmental contributors (medications, airflow, dust, debris, contact lenses or toxins)
(2) lid malposition inducing poor tear coverage (entropion, ectropion,, trichasis, symblepheron and lagophthalmos)
(3) globe-affecting pathologies moving the eye in the orbit, creating a coverage anomaly or volume shortage (tumor, thyroid dysophthalmopathy)
Dysfunction of the lipid-producing glands provokes evaporative dry eye. Blepharitis produces lipases which hydrolyze cholesterol esters creating fatty acids and increased tear evaporation. Free fatty acids are toxic to the corneal epithelium, resulting in epitheliopathy and inflammation (meibomian gland dysfunction or MGD).11
Aqueous deficiency—subnormal lacrimal gland production—is related to age (hormonal and homeostatic remodeling). Inflammatory processes from systemic disease (sarcoidic infiltration) or autoimmunity (Stevens-Johnson) can also slow tear secretion.22-24 Gender/hormonal fluctuations in estrogen and progesterone diminish lacrimal gland stimulation in women.22-24 Medications including antihistamines, beta blockers, antidepressants and diuretics also are implicated.25-27 Obstructed lacrimal ducts due to scarring (cicatricial pemphigoid, trachoma and chemical/radiation exposure) are also known offenders.11-20 Neurological gland block (tumors, trauma, vascular accidents or ischemic vascular disease) can also stop tear production.
Mucus deficiency arises secondary to all of the above-named etiologies. Mucus lowers the wetting coefficient, permitting tears to couple with the epithelium.28-30
Patient Evaluation & Treatment
Workup for dry eye includes a through history (environmental issues, contact lens history, medications, present illness, exacerbating factors, relieving factors and attempted treatments). Examination includes tear break-up time to assess lipids, lacrimal lake observation, tear volume testing (phenol red thread or Schirmer test strip) and sodium fluorescein evaluation of the cornea.31 In cases of suspected systemic disease, laboratory testing or imaging may be appropriate.
Treatment is aimed at resolving the root cause and symptomatology. The TFOS Dry Eye Workshop and Delphi Panel suggest a stepped approach in accordance with the underlying pathology.32-39 For aqueous deficient dry eyes, tear supplementation or salivatory stimulation can increase tear volume.31 Patients with exposure keratopathy require thicker emollients and ointment at bedtime. Stimulating the lacrimal gland with topical cyclosporine while reducing inflammation via topical steroidal therapy is effective.40-44 Patients with filamentary findings or morning syndrome (abrasion upon waking) may benefit from nocturnal soft lens bandaging.45 Patients with blepharitis or MGD can be treated with topical and oral antibiotics (tetracyclines), lid scrubs and warm compresses.11,46 Oral nutritional supplements (omega-3 fatty acids) can supply tear-building blocks and augment mucus-producing capability. Punctal plugs, cautery, gold weight installation and tarsorraphy are advanced considerations.47-54
Ocular surface disease is a complicated process requiring thoughtful investigation. Most cases require reevaluation and monitoring to prevent evolving surface disease. This patient was placed on topical tear supplementation therapy OU. Recognizing that the oral antihistamine was necessary to alleviate to ear issue, it is not be discontinued.
Dr. Gurwood thanks Dr. Balachandran for contributing this case.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
|
1. Stoeckelhuber M, Stoeckelhuber BM, Welsch U. Human glands of Moll: histochemical and ultrastructural characterization of the glands of Moll in the human eyelid. J Invest Dermatol. 2003;121(1):28-36. 2. Van Santvliet L, Ludwig A. Determinants of eye drop size. Surv Ophthalmol. 2004;49(2):197-213. 3. Francisco FC, Carvalho AC, Francisco VF et al. Evaluation of 1000 lacrimal ducts by dacryocystography. Br J Ophthalmol. 2007;91(1):43-46. 4. Oyster CW. The eyelids and the lacrimal system. In: Oyster, C.W. The Human Eye Structure and Function. Sunderland Massachusetts, Sinauer Associates, Inc.: 291-320. 5. Johnson ME, Murphy PJ. Temporal changes in the tear menisci following a blink. Experimental Eye Research. 2006;83(3):517-525. 6. Sahlin, S, Chen E, Kaugesaar T, et al. Effect of eyelid Botulinum toxin injection on lacrimal drainage. Am J Opthalmol. 2000;129(4):481-486. 7. Zhuang L, Sylvester CL, Simons JP. Bilateral congenital lacrimal fistulae: a case report and review of the literature. Laryngoscope. 2010;120 Suppl 4:S230. 8. Skorin L Jr. A review of entropion and its management. Cont Lens Anterior Eye. 2003;26(2):95-100. 9. Eliasoph I. Current techniques of entropion and ectropion correction. Otolaryngol Clin North Am. 2005;38(5):903-19. 10. Vallabhanath P, Carter SR. Ectropion and entropion. Curr Opin Ophthalmol. 2000;11(5):345-51. 11. Knop E, Knop N.Meibomian glands : part IV. Functional interactions in the pathogenesis of meibomian gland dysfunction (MGD). Ophthalmologe. 2009;106(11):980-7. 12. Lee SY, Petznick A, Tong L. Associations of systemic diseases, smoking and contact lens wear with severity of dry eye. Ophthalmic Physiol Opt. 2012;32(6):518-26. 13. Lois N, Abdelkader E, Reglitz K, Garden C, Ayres JG. Environmental tobacco smoke exposure and eye disease. Br J Ophthalmol. 2008;92(10):1304-10. 14. Anwar Z, Wellik SR, Galor A. Glaucoma therapy and ocular surface disease: current literature and recommendations. Curr Opin Ophthalmol. 2013;24(2):136-43. 15. Askeroglu U, Alleyne B, Guyuron B. Pharmaceutical and herbal products that may contribute to dry eyes. Plast Reconstr Surg. 2013;131(1):159-67. 16. Sun Z, Hong J, Liu Z et al. Coal dust contiguity-induced changes in the concentration of TNF-alpha and NF-kappa B p65 on the ocular surface. Ocul Immunol Inflamm. 2009;17(2):76-82. 17. Mameletzi E, Hamedani M, Majo F, Guex-Crosier Y. Clinical manifestations of mucous membrane pemphigoid in a tertiary center. Klin Monbl Augenheilkd. 2012;229(4):416-9. 18. Wolle MA, Cassard SD, Gower EW, et al. Impact of trichiasis surgery on physical functioning in Ethiopian patients: STAR trial. Am J Ophthalmol. 2011;151(5):850-7. 19. Bernardes TF, Bonfioli AA. Blepharitis. Semin Ophthalmol. 2010;25(3):79-83. 20. Patel V, Daya SM, Lake D, Malhotra R. Blink lagophthalmos and dry eye keratopathy in patients with non-facial palsy: clinical features and management with upper eyelid loading. Ophthalmology. 2011;118(1):197-202. 21. Kırımlıoğlu H, Takmaz T, Can I. et al. Ocular surface and dry eye in Graves' disease. Curr Eye Res. 2011;36(1):8-13. 22. Rocha EM, Mantelli F, Nominato LF, Bonini S. Hormones and dry eye syndrome: an update on what we do and don't know. Curr Opin Ophthalmol. 2013;24(4):348-55. 23. Sullivan DA, Sullivan BD, Evans JE, et al. Androgen deficiency, meibomian gland dysfunction, and evaporative dry eye. Acad Sci. 2002 ; 966:211-22. 24. Sullivan DA, Sullivan BD, Ullman MD, et al. Androgen influence on the meibomian gland. Invest Ophthalmol Vis Sci. 2000;41(12):3732-42. 25. Askeroglu U, Alleyne B, Guyuron B. Pharmaceutical and herbal products that may contribute to dry eyes. Plast Reconstr Surg. 2013;131(1):159-67. 26. Moss SE, Klein R, Klein BEK. Prevalence of and risk factors for dry eye syndrome. Arch Ophthalmol. 2000;118(9):1264-1268. 27. Izazola-Conde C, Zamora-de la Cruz D, Tenorio-Guajardo G. Ocular and systemic adverse effects of ophthalmic and non ophthalmic medications. Proc West Pharmacol Soc. 2011;54:69-72. 28. Watanabe H. Significance of mucin on the ocular surface. Cornea. 2002;21(2 Suppl 1):S17-22. 29. Gipson IK. Distribution of mucins at the ocular surface. Exp Eye Res. 2004;78(3):379-88. 30. Gipson IK, Hori Y, Argüeso P. Character of ocular surface mucins and their alteration in dry eye disease. Ocul Surf. 2004;2(2):131-48. 31. Pramanik T, Ghising R. Salivation induced better lacrimal gland function in dry eyes. Nepal Med Coll J. 2009;11(4):258-60. 32. International Dry Eye WorkShop study group. The definition and classification of dry eye disease: report of the Definition and Classification Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):75-92. 33. International Dry Eye WorkShop study group. The epidemiology of dry eye disease: report of the Epidemiology Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):93-107. 34. International Dry Eye WorkShop study group. Methodologies to diagnose and monitor dry eye disease: report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):108-52. 35. International Dry Eye WorkShop study group. Design and conduct of clinical trials: report of the Clinical Trials Subcommittee of the International Dry Eye Workshop. Ocul Surf. 2007;5(2):153-62. 36. International Dry Eye WorkShop study group. Management and therapy of dry eye disease: report of the Management and Therapy Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):163-78. 37. International Dry Eye WorkShop study group. Research in dry eye: report of the Research Subcommittee of the International Dry Eye WorkShop. Ocul Surf. 2007;5(2):179-93. 38. Behrens A, Doyle JJ, Stern L, et al. Dysfunctional tear syndrome: a Delphi approach to treatment recommendations. Cornea. 2006;25(8):900-7. 39. Wilson SE, Stulting RD. Agreement of physician treatment practices with the international task force guidelines for diagnosis and treatment of dry eye disease. Cornea. 2007;26(3):284-9. 40. Prabhasawat P, Tesavibul N, Mahawong W. A randomized double-masked study of 0.05% cyclosporine ophthalmic emulsion in the treatment of meibomian gland dysfunction. Cornea. 2012;31(12):1386-93. 41. Demiryay E, Yaylali V, Cetin EN, Yildirim C. Effects of topical cyclosporine a plus artificial tears vs. artificial tears treatment on conjunctival goblet cell density in dysfunctional tear syndrome. Eye Contact Lens. 2011;37(5):312-5. 42. Perry HD, Donnenfeld ED. Topical 0.05% cyclosporin in the treatment of dry eye. Expert Opin Pharmacother. 2004;5(10):2099-107. 43. Utine CA, Stern M, Akpek EK. Clinical review: topical ophthalmic use of cyclosporin A. Ocul Immunol Inflamm. 2010;18(5):352-61. 44. Donnenfeld E, Pflugfelder SC. Topical ophthalmic cyclosporine: pharmacology and clinical uses. Surv Ophthalmol. 2009;54(3):321-38. 45. Albietz J, Sanfilipo P, Troutbeck R, Lenton LM. Management of filamentary keratitis associated with aqueous-deficient dry eye. Optom Vis Sci. 2003;80(6):420-30. 46. Foulks GN, Nichols KK, Bron AJ, et al. Improving awareness, identification, and management of meibomian gland dysfunction. Ophthalmology. 2012;119(10 Suppl):S1-12. 47. Tai MC, Cosar CB, Cohen EJ, Rapuano CJ, Laibson PR. The clinical efficacy of silicone punctal plug therapy. Cornea. 2002;21(2):135-9. 48. Holzchuh R, Villa Albers MB, Osaki TH, et al. Two-year outcome of partial lacrimal punctal occlusion in the management of dry eye related to Sjögren syndrome. Curr Eye Res. 2011;36(6):507-12. 49. Ohba E, Dogru M, Hosaka E, et al. Surgical punctal occlusion with a high heat-energy releasing cautery device for severe dry eye with recurrent punctal plug extrusion. Am J Ophthalmol. 2011;151(3):483-7. 50. Rofagha S, Seiff SR. Long-term results for the use of gold eyelid load weights in the management of facial paralysis. Plast Reconstr Surg. 2010;125(1):142-9. 51. Bergeron CM, Moe KS. The evaluation and treatment of upper eyelid paralysis. Facial Plast Surg. 2008;24(2):220-30. 52. Tan ST, Staiano JJ, Itinteang T, et al. Gold weight implantation and lateral tarsorrhaphy for upper eyelid paralysis. J Craniomaxillofac Surg. 2013;41(3):e49-53. 53. de Silva DJ, Ramkissoon YD, Ismail AR, Beaconsfield M. Surgical technique: modified lateral tarsorrhaphy. Ophthal Plast Reconstr Surg. 2011;27(3):216-8. 54. Kazim M, Gold KG. A review of surgical techniques to correct upper eyelid retraction associated with thyroid eye disease. Curr Opin Ophthalmol. 2011;22(5):391-3. |
