 |
Binocular vision and accommodative issues are prevalent in most patient populations. In a population of optometry students, one study found that the prevalence of non-strabismic accommodative dysfunction was 55%, vergence dysfunction was 73% and oculomotor dysfunction was 15%.1 Another study investigated university students’ vision and found that 32.3% showed general binocular dysfunction.2 In a population of Australian children from a remote village, one study found that 15% had binocular vision or accommodative disorders.3
While all of these issues can benefit from treatment that includes vision therapy, several of them may also benefit from the addition of plus lenses. These can potentially help with accommodative insufficiency, convergence excess and basic esophoria.
While it is lovely when numbers line up perfectly to diagnose these conditions, another way to decide whether plus at near will be valuable to the patient is to look at the examination data. The following findings indicate that plus at near may be an effective addition to treatment: high AC/A, esophoria at near, low positive relative accommodation (PRA), high monocular estimation method (MEM) or fused cross-cylinder test (lag of accommodation), low amplitude of accommodation and failing minus on accommodative facility. Plus at near can be given either for near vision only, or as a bifocal if the patient has a distance prescription or is unwilling to take their glasses off for near viewing.
Believe it or not, some patients, especially teens and young adults, do not like wearing reading glasses or bifocals. Even though there are visual advantages, the emotional and psychosocial aspects of wearing glasses with a line, or what may be deemed “granny glasses,” sometimes outweigh those benefits for patients. In such cases, we have progressive addition lenses, but another option to consider is contact lenses. There are several bifocal contact lens designs to weigh, of which some will be described in two case reports below.
Case 1
An 18-year-old female college student presented with complaints of headaches and eye strain with extended reading and computer work that started upon entering college several months prior. She was a graphic design major, which required her to spend extended time on the computer. She wore contact lenses (-3.00D OU, Bausch + Lomb Ultra sphere) and had worn glasses since age 12. Her acuity with contacts was 20/20 OD, OS, OU at distance and 20/25 OD, OS, OU at near. Her cover test was ortho at distance and three esophoria at near. Stereopsis was 40 seconds of arc and negative relative accommodation (NRA) and PRA was unbalanced at +2.50/-0.50. The base-out vergence at near showed normal blur and break but poor recovery. Near point of convergence was “to the nose” x 3.
The patient was trial framed at near with +1.00D over her habitual contact lenses. Her visual acuity sharpened to 20/20 OU at near, the cover test at near was measured at three exophoria and stereopsis was 25 seconds of arc; she was diagnosed with convergence excess. She was presented with two treatment options, including plus readers over her contact lenses or bifocal contact lenses—she chose the latter.
 |
|
The Ultra multifocal is designed to fit different add powers as well as levels of astigmatism. Photo: Bausch + Lomb. Click image to enlarge. |
Fortunately, the Ultra family of contact lenses from Bausch + Lomb (B+L) includes a multifocal option with a variety of features, including low vs. high add powers and astigmatism up to -2.75DC. The low add ranges from +0.75D to +1.50D and the high add from +1.75D to +2.50D. With the Ultra sphere and multifocal both having the same base curve (8.5mm) and diameter (14.2mm), it was an easy switch to the multifocal version with a low add OU for this patient. The final contact lens prescription was B+L Ultra multifocal -3.00DS/+1.00 add OU. This refinement provided the clear distance and comfortable near vision that the patient required for her schoolwork. Upon follow-up, she reported that her symptoms had abated and she could function symptom-free throughout the day.
Case 2
A 12-year-old girl presented with complaints of words moving on the page or screen and blurry vision when looking too long at near. She wore glasses since the age six, with a current Rx of -3.00-3.25x180 OD and -2.50-4.00x180 OS. Her corrected visual acuity was 20/25 OD, OS, OU at distance and 20/30 OD, OS, OU at near. Her cover test was ortho at distance and three exophoria at near; stereopsis was 60 seconds of arc. A subjective refraction found a small increase in myopia (-3.25-3.25x180 OD and -2.75-4.00x180 OS). NRA and PRA was unbalanced at +2.00/-0.25. Accommodative amplitudes were 8.00D OD, OS and the MEM was +1.25D OD, OS.
The patient was trial framed at near with +0.75D over her new prescription. Her visual acuity sharpened to 20/20 OU, the MEM was +0.75D and stereopsis was 20 seconds of arc. She was consequently diagnosed with accommodative insufficiency and given two treatment options: a bifocal in her glasses, either as a flat top or progressive addition lens, or a bifocal contact lens. She exuberantly chose the latter.
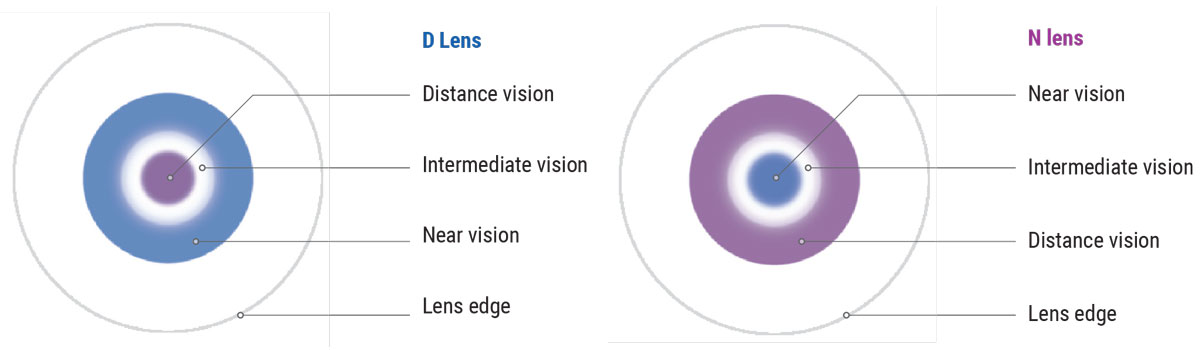
Although this patient’s high cylinder and need for a multifocal contact lens could have certainly been intimidating, only one non-customizable, stock option exists on the market that corrects cylinder greater than -2.75DC. Fortunately, it is a great one! The Biofinity family from CooperVision includes a multifocal option with a variety of features, including four add powers (+1.00, +1.50, +2.00, +2.50), inclusion of astigmatism up to -5.75DC and specification of a center-distance (CD) vs. center-near design. After vertexing, the appropriate trial lenses to order were -3.25-2.75x180/+1.00 add/CD OD and -2.75-3.75x180/+1.00 add/CD OS.
 |
|
The Biofinity multifocal comes in two different lens designs, center-distance (left) or center-near (right). Photo: CooperVision. Click image to enlarge. |
At the fitting, the lenses were sitting appropriately and did not rotate. Her vision was 20/20 OD, OS, OU at distance and at near. The MEM was measured at +0.50 and the accommodative amplitudes were 12D OD, OS. The patient was subsequently scheduled for a follow-up appointment in three months. This would determine whether near visual symptoms improved and exam data continued to be stable. If they are, the add power may be increased to +1.50 OU in order to provide a minor amount of myopia control to reduce myopic progression.
Discussion
Multifocal contacts are a wonderful option for patients who need plus at near to treat accommodative and vergence issues. With the advancement of contact lens technology and production, it is becoming safer and more comfortable for young patients with accommodative insufficiency, convergence excess and basic esophoria to be fit into them. Although the lenses can be intimidating to fit initially, there are only a handful of multifocal options on the market—and only two with astigmatism correction. The only pieces of data that the practitioner needs are an accurate binocular balance prescription and a determination of the desired add power to get started. Patients will be thrilled—socially and emotionally—for this treatment option, while having their symptoms addressed at the same time. This is a win-win scenario for all parties.
We would like to thank Chawan Rasheed, OD, assistant professor of optometry at Southern College of Optometry, for assisting with the contact lens aspects of this column.
Dr. Taub is a professor and co-supervisor of the Vision Therapy and Pediatrics residency at Southern College of Optometry (SCO) in Memphis. He specializes in vision therapy, pediatrics and brain injury. Dr. Schnell is an associate professor at SCO and teaches courses on ocular motility and vision therapy. She works in the pediatric and vision therapy clinics and is co-supervisor of the Vision Therapy and Pediatrics residency. Her clinical interests include infant and toddler eye care, vision therapy, visual development and the treatment and management of special populations. They have no financial interests to disclose.
1. Dahal M, Khatri B. Prevalence of non-strabismic binocular vision dysfunction among optometry students in Bangalore, India. Optom Vis Perform. 2019;7(1):23-7. 2. Read SA, Hopkins S, Black AA, et al. Prevalence of vision conditions in children in a very remote Australian community. 2022;106(2):195-201. 3. Porcar E, Martinez-Palomera A. Prevalence of general binocular dysfunctions in a population of university students. Optom Vis Sci. 1997;74(2):111-3. |
