 |
The body’s peripheral vascular network is composed of arteries, veins and capillaries, each of which exhibit unique characteristics contributing to their function. The eye, like every other organ in the body, contains both an arterial and a venous system in order to adequately deliver oxygen and nutrients to and from ocular structures and eliminate waste. Regardless of which organ is discussed, all blood vessels throughout the body possess similar anatomical properties. Identifying their distinguishing anatomical features makes us one step closer to understanding the various ocular pathologies that arise as a result of systemic vascular disorders.1,2
Complementary Function
Arteries, or arterioles, are responsible for transporting blood to the eye for nourishment. This occurs through the internal carotid artery, which extends from the heart and branches into the ophthalmic artery. The ophthalmic artery further subdivides into the internal carotid artery, the long and short posterior ciliary arteries and the anterior ciliary arteries. This arterial network supplies the various anterior and posterior ocular structures with oxygen and nutrients. Veins perform the opposite function, in that they return blood from a given structure back to the heart. Venous outflow is mediated by the central retinal vein and vortex veins, which are branches of the superior and inferior ophthalmic veins. They ultimately drain through structures such as the cavernous sinus, pterygoid venous plexus and facial vein.3 These anatomical connections explain why ocular diseases spread throughout different compartments of the head and neck.
 |
|
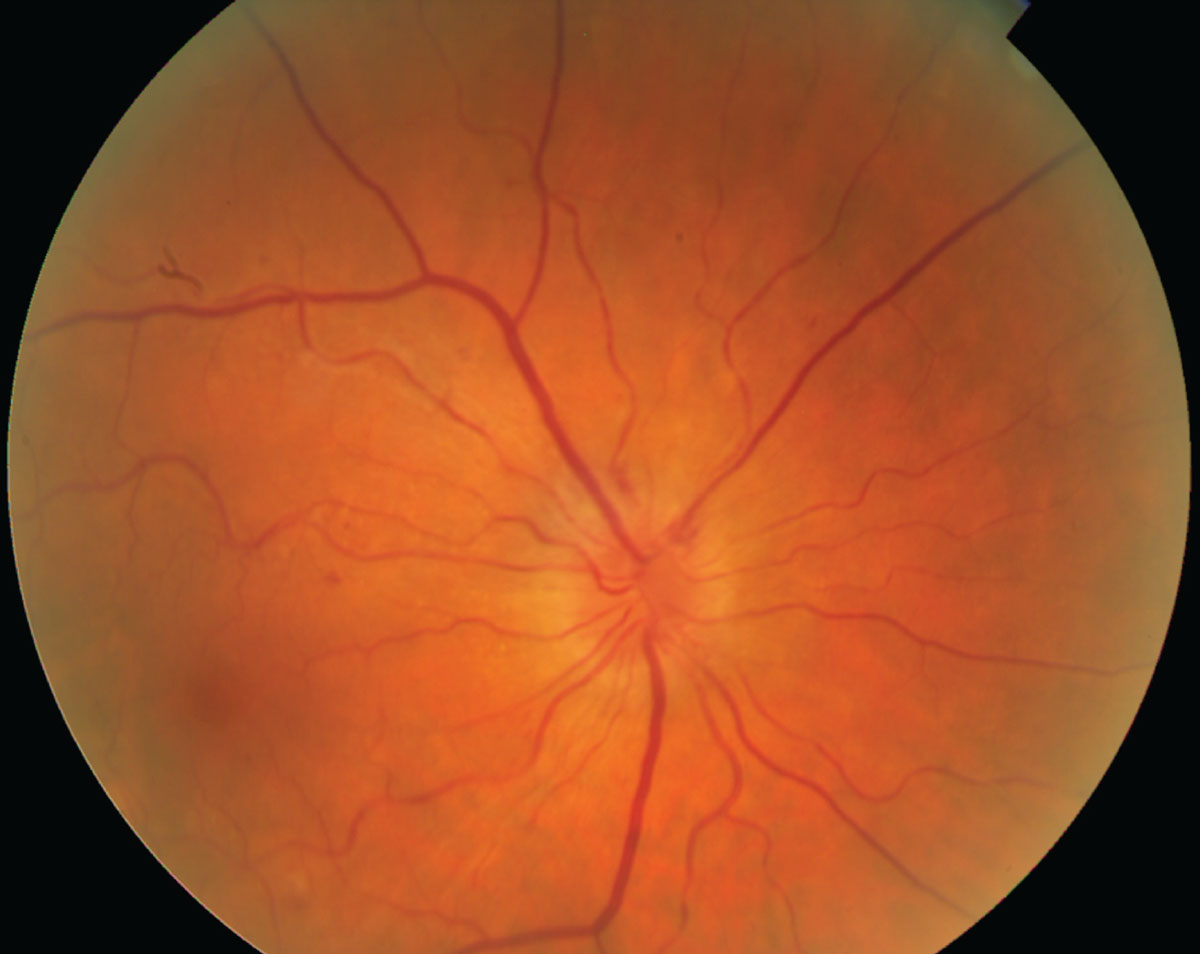
Hypertensive retinopathy causing constriction of retinal arterioles in response to elevated systemic blood pressure and autoregulation. Click image to enlarge. |
An illustration of arterial function is the case of retinal artery occlusion, where blood is prevented from perfusing the retina due to an obstruction of an artery. As such, the area in which the occluded artery is responsible for perfusing appears whitened and ischemic, due to lack of blood flow. In contrast, if a retinal vein occlusion occurs, blood is prohibited from leaving the retina, and severe hemorrhages form in the area of distribution of the affected vein.
Divergent Purposes
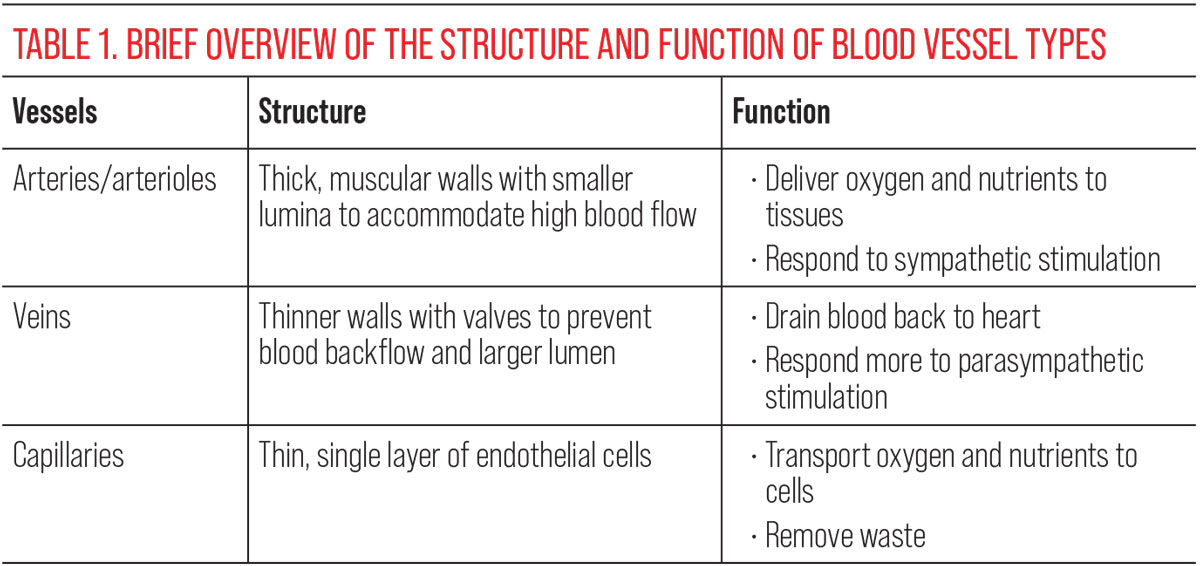
While arteries and veins share some structural similarities, they also have notable anatomical differences that affect their functions. One of the most significant differences is the thickness and elasticity of their walls. Arteries have thicker, more muscular walls that allow them to withstand the high pressure of blood flow from the heart. Veins, however, have thinner walls with less muscle and are not designed to withstand high pressure. Instead, they have valves that prevent blood from flowing backward. This makes veins particularly sensitive to hematological factors such as hypercoagulability or vasculitides, which are often underlying factors in retinal vein occlusions.4,5
Another major difference between arteries and veins is their size. Arteries have smaller lumina than veins, which means that blood flows through them more quickly. This is because arteries are designed to transport oxygenated blood away from the heart to the rest of the body at high pressure. In contrast, veins have larger lumina and slower blood flow, as they are designed to return deoxygenated blood from the body back to the heart. When observing retinal vasculature, for example, a normal ratio between arteries and veins is 2:3; this ratio is often reduced in systemic disease processes that affect vessel attenuation.5
Arteries and veins also respond differently to neurotransmitters and hormones. Arteries are more responsive to sympathetic nervous system stimulation, which can cause them to constrict and increase blood pressure. Veins are more responsive to parasympathetic nervous system stimulation, which can cause them to dilate and decrease blood pressure. This distinction is due to the differences in their smooth muscle cell composition. These features are clinically relevant in that arteries are more susceptible to elevations in blood pressure, causing them to initially constrict in response and manifest as the arteriolar narrowing that is often observed in any stage of hypertensive retinopathy.4-7
 |
| Click image to enlarge. |
In addition to arterioles and veins, there are choriocapillaris and capillaries located in the retina. Due to the high metabolic demands of retinal cells, these tiny blood vessels provide additional oxygen and nutrients. The choriocapillaris supplies the outer retinal layers in particular, whereas the retinal capillaries supply the inner portion. These capillaries are also responsible for removing waste products from the retina and transporting them into the bloodstream for elimination from the body. The structure of a capillary is a thin, single layer of endothelial cells, allowing diffusion of nutrients. Capillary function is implicated in many disease processes that lead to nonperfusion or growth of neovascularization.2,6
Arteries, veins and capillaries have a number of anatomical differences that affect their function. These include differences in wall thickness, structure, oxygenation status and responsiveness to neurotransmitters and hormones. Understanding these differences is important for understanding how blood circulates through the eye and how it is susceptible to systemic vascular diseases.
Dr. Labib graduated from Pennsylvania College of Optometry, where she now works as an associate professor. She completed her residency in primary care/ocular disease and is a fellow of the American Academy of Optometry and a diplomate in the Comprehensive Eye Care section. She has no financial interests to disclose.
1. Mercadante AA, Raja A. Anatomy, arteries. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2023. Updated March 6, 2023. 2. Tucker WD, Arora Y, Mahajan K. Anatomy, blood vessels. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. 2022. Updated August 8, 2022. 3. Kiel JW. The ocular circulation. San Rafael (CA): Morgan & Claypool Life Sciences. 2010. 4. Tortora GJ, Derrickson BH. Principles of anatomy and physiology. John Wiley & Sons. 2017. 5. Boron WF, Boulpaep EL. Medical physiology. Elsevier Saunders. 2016. 6. Hall JE, Hall, ME. Textbook of medical physiology. Elsevier Saunders. 2015. 7. Widmaier EP, Raff H, Strang KT. Vander’s human physiology: the mechanisms of body function. McGraw-Hill. 2014 |
