 |
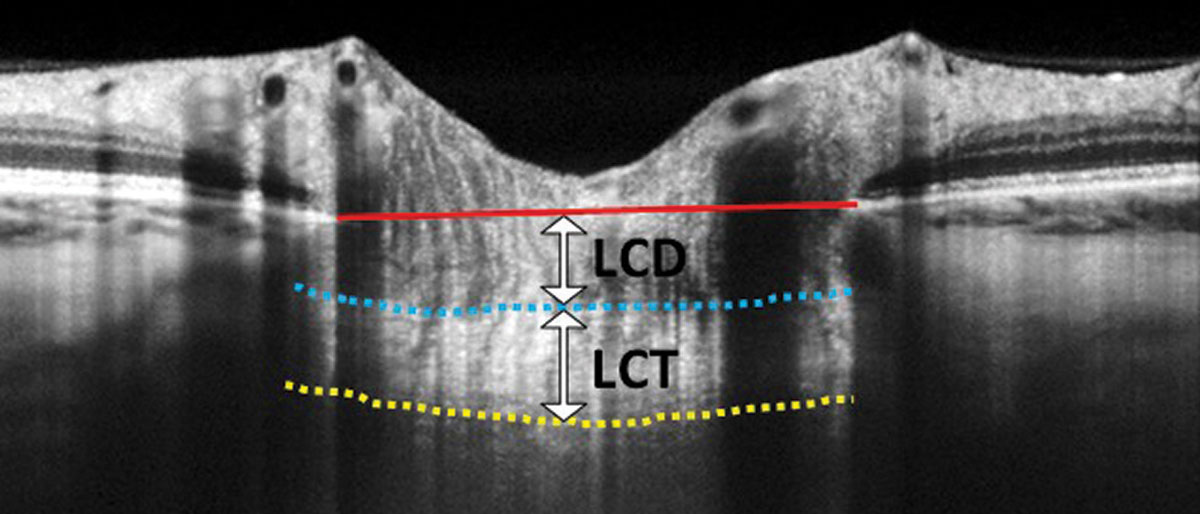
| Researchers found a lower lamina cribrosa thickness (LCT) in patients whose visual field showed a parafoveal scotoma. In the above EDI-OCT scan, LCT is measured from the anterior border (blue dashed line) to the posterior border (yellow dashed line) of the lamina cribrosa. Lamina cribrosa depth (LCD) is measured along a perpendicular line from the anterior border of the lamina to a reference line that connects the edges of Bruch’s membrane (red solid line). Photo: Carolyn Majcher, OD. Click image to enlarge. |
The researchers of a new retrospective study aimed to investigate how patterns of visual field loss in normotensive glaucoma (NTG) might illuminate our understanding of the affected areas of the optic nerve head in the disease’s course. As such, they analyzed correspondence of lamina cribrosa (LC) morphology in NTG patients with visual field defects’ location.
A total of 96 eyes from 96 NTG patients were observed. Participants were divided into two groups depending on visual field defect location, either parafoveal scotoma (PFS) or peripheral nasal step (PNS). OCT was used to look at the optic disc and swept-source OCT for the macula. The two groups were then compared for optic disc, macula, LC and connective tissues.
What the researchers found was that the temporal peripapillary retinal nerve fiber layer, average macular ganglion cell inner plexiform layer and average macular ganglion cell complex were all thinner in those with PFS that for those with PNS. Additionally, the former group also saw more glaucomatous LC morphology with a smaller LC global shape index, more LC defects, and a thinner LC than the other group.
Based on these observations, the researchers of the study believe “the morphological differences in LC may be related with the initial location of visual field defects.”
The researchers then outlined what previous research has already shown in relation to their findings. Of note, one prior study reported a thinner LC in NTG vs. primary open-angle glaucoma patients, while another study saw unilateral NTG eyes with a thinner LC than the fellow eye with normal optic disc morphology. In the same study, the fellow eye of NTG patients was had thinner LC than control eyes.
More research has indicated that visual field defects and their locations may be influenced by vascular risk factors for glaucoma patients. One study found initial PFS in glaucoma patients was correlated with greater prevalence of systemic vascular risk factors like migraine, hypotension and sleep apnea, when compared with initial PNS presentation.
Another study pointed to by the researchers found narrower retinal arteriolar diameter in patients with open-angle glaucoma with initial PFS compared with those with initial PNS. IOP-independent factors are thought to potentially be the cause leading to initial PFS, since the papillomacular bundle related to PFS is vulnerable to ischemic damage, something like abnormal ocular blood flow could damage the retinal nerve fiber layer close to said papillomacular bundle in early-staged glaucoma.
Based on this and other previous research, the study authors believe their findings indicate vascular dysfunction of these glaucoma patients. They consequently state that “considering these facts and the limitations of treatment for the improvement of vascular dysfunction, it is advisable that IOP should be lower in NTG patients with initial PFS than in those with initial PNS.”
Kang YS, Haowei Z, Sung MS, Park SW. Lamina cribrosa morphology in normal-tension glaucoma according to the location of visual field defects. J Glaucoma. March 6, 2023. [Epub ahead of print]. |