 |
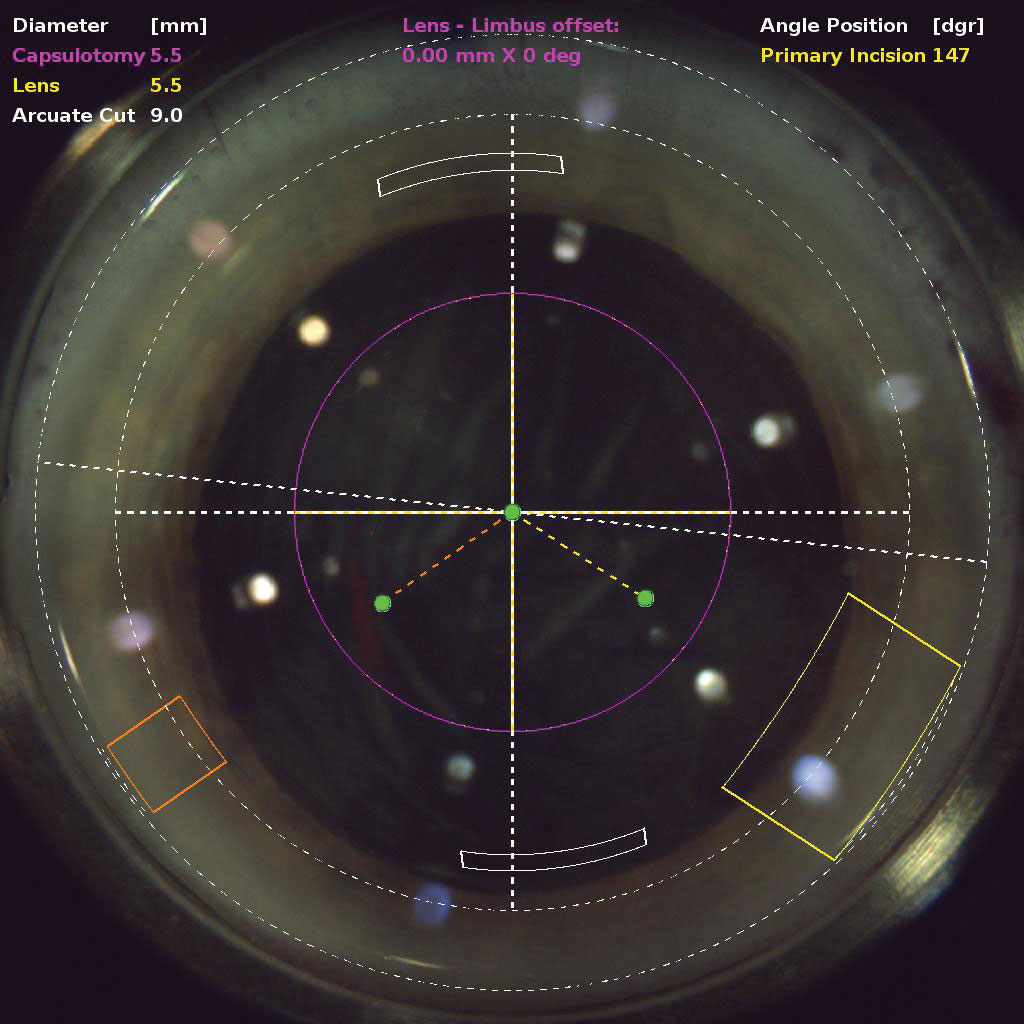
| A robust health economics analysis in France found that femtosecond laser-assisted cataract surgery in its current state of development was not cost-effective. Photo: Justin Schweitzer, OD. Click image to enlarge. |
Femtosecond laser-assisted cataract surgery (FLACS) has often been touted as a breakthrough in improving surgical outcomes, with well-documented efficacy and safety. Nevertheless, an important requirement for surgeons, insurers and other stakeholders is the evaluation of its cost-effectiveness over a sufficiently long horizon. A recent analysis published in JAMA Ophthalmology compared FLACS with traditional phaco-based cataract surgery over 12 months and found that the former was not within the $50,000 to $150,000 per quality-adjusted life-year (QALY) range frequently cited as cost-effective in the United States.1 QALY is a measure of patient quality of life that takes into account the likely remaining lifespan of the individual in assessing the value of a medical intervention.
Evaluating the cost-effectiveness of this treatment was actually a secondary objective of the Economic Evaluation of Femtosecond Laser-Assisted Cataract Surgery study, a multicenter, participant-masked, randomized clinical trial conducted in France. All patients eligible for unilateral or bilateral cataract surgery 22 and older were included. Of 870 randomized patients, 62.4% were female, and the mean age at surgery was 72.3. A total of 440 patients were randomized to receive femto cataract surgery and 430 to receive the traditional version. The rate of bilateral surgery was 63.3%.
The mean costs of cataract surgery—in a European setting not directly comparable to the US—were $1,235 for femto laser and $621 for phaco. The total mean cost of care at 12 months was $7,787 for participants treated with femto laser and $7,146 for participants treated with phaco. FLACS yielded a mean of 0.788 QALY, and phaco yielded 0.792 QALY. The difference in mean costs was $600, and the difference in QALY was -0.004. The incremental cost-effectiveness ratio was $150,000 per QALY. The cost-effectiveness probability of femto laser compared with phaco was 15.7% for a cost-effectiveness threshold of $32,973 per QALY.
“A cost-utility analysis may not necessarily reflect the results observed on an efficacy endpoint but rather provide additional information on the benefits of a healthcare intervention to decision-makers,” the authors emphasized in their paper. “Femtosecond laser–assisted cataract surgery in its current state of development was not cost-effective and should not be reimbursed by healthcare systems,” they concluded. “Nonetheless, investment in research and development is worthwhile, and more advanced femtosecond laser may represent a valuable option in cataract surgery in the future.”1
A commentary also published in JAMA Ophthalmology remarked on the findings. “Sometimes, when two drugs are equivalent in efficacy, one might still be considered superior based on a lower adverse effect profile, reduced cost or perhaps a shorter treatment course,” wrote the commentary author, prominent Johns Hopkins ophthalmologist Oliver Schein, MD. “However, when two surgical procedures are equivalent in rates of both favorable clinical outcomes and complications, there is only one obvious conclusion when one costs more.”2
He pointed out that, in many practices, patients are flooded with messaging—some overt and some indirect—that the choice of femto laser over phaco is one of premium vs. ordinary or optimal vs. acceptable. Sometimes these messages are conflated, at least in patients’ minds, with intraocular lens choices. He believed that the prevalence of such messaging and its misunderstanding raises concerns about professionalism.
“Given the results of the research by our colleagues in France, it remains unlikely that femto laser in its current incarnation would be funded by federal or private insurers in the United States. Ironically, were that to happen, the rate of this procedure in the United States would likely fall precipitously,” Dr. Schein concluded. “From the perspective of the surgeon, an extra $300 per case would probably not justify the extra time and expense of femto laser, especially in the known absence of clinical benefit.”2
1. Bénard A, Sitta R, Brezin AP, et al. Cost utility and value of information analysis of femtosecond laser–assisted cataract surgery. JAMA Ophthalmol. May 18, 2023. [Epub ahead of print]. 2. Schein OD. Femtosecond laser-assisted cataract surgery—conclusive evidence of lack of incremental value. JAMA Ophthalmol. May 18, 2023. [Epub ahead of print]. |