 |
An estimated 20.5 million Americans already have cataracts, and this number is expected to increase to 30.1 million by 2020.1 Indeed, cataract surgery is the most frequently performed surgical procedure among Medicare beneficiaries.2
Those among this group who undergo cataract surgery will likely find the improvement in color and contrast sensitivity to be somewhat dramatic. However, corneal aberrations also are likely to increase after IOL implantation.3
Imagine the possibility of offering enhanced vision thats comparable to that of younger patients, improving vision in dim illumination and eliminating aberrations. Research and development of aspheric IOLs may make these possibilities more of a reality for patients.
New Models
Researchers developed a mathematical eye model based on a six-surface eye model developed by Swedish ophthalmologist Allvar Gullstrand (1862-1930). Dr. Gullstrand won the Nobel Prize in Physiology or Medicine in 1911 for research about how optical images form in the eye. For his six-surface eye model, which he developed in 1909, he used geometrical ray tracing techniques to exhibit three-point aberrations (spherical aberration, coma, astigmatism) of the eye and when possible, make a comparison with the response of an actual eye.4
The researchers mentioned above modified Dr. Gullstrands model according to clinically measured aspheric data and by compensating for high-resolution imaging to study human eye aberrations. They found that spherical aberration and defocus (myopia or hyperopia) were the most significant aberrations for on-axis imaging, while a combination of oblique astigmatism, coma, spherical aberration and defocus was most significant for off-axis imaging.5 On-axis imaging refers to a point source that focuses directly through the visual axis and onto the macula. Off-axis refers to stray light that is imaged from the peripheral cornea; it is still significant, however, and still focuses on the retina.
Given this research, aspheric IOLs may offer improved optical performance following cataract surgery.
Aspheric optics allow us to visualize an object in a flat plane as opposed to a curved appearance. The object is seen as normalas it should be either curved or flat. A spherical lens, however, changes a flat object, for example, and makes it appear curved, or the lens makes a curved object appear more curved. In figure one, for example, each object light ray focuses into one image plane vs. spherical optics, in which each point might focus in a different place.6
| Spherical | Aspheric |
 |
| 1. In aspheric optics, each object light ray focuses into one image plane vs. spherical optics, in which each point might focus in a different place. |
Each of us has some degree of corneal spherical aberration simply due to the fact that our peripheral cornea is flatter than the central cornea, and we get more bending of light in the periphery.7 At birth, the eyes crystalline lens has a negative asphericity. This negative asphericity neutralizes the natural positive asphericity of the cornea. As we age, however, the lens thickens and becomes positively aspheric.8 This explains why many patients start to see halos around lights as their cataracts progress. Perhaps in the future we might gauge the severity of a cataract by measuring spherical aberration.
Aspheric optics are not new to optometry. For example, we employ aspheric optics whenever we use condensing lenses for ophthalmoscopy and even when we use the slit lamp.9 High-quality spectacles, fundus cameras and new contact lenses can correct for spherical aberration.
IOL Technology
Besides the applications mentioned above, aspheric optics have become a part of IOL technology. Specifically, aspheric IOLs can correct spherical aberration, thus offering improved optical performance compared to traditional IOLs.10
One group of German researchers designed a 22.00D aspheric IOL.10 Hoping to improve the optical performance up to the limit of diffraction, they changed the second radius of the lens to cover a larger range of needed refractive power. They found that the spot size enlarged as expected, but it was considerably smaller than that of the respective spherical IOL, and the image quality was considerably better than the respective spherical IOL.
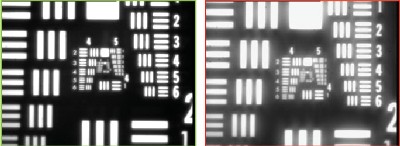
| B&L SofPort AO | Traditional IOL |
 |
|
2. Researchers have found variation in vision quality between an IOL with aspheric optics vs. a standard IOL. |
One advantage of the neutral aspheric design: Any slight decentration of the IOL does not dramatically alter the quality of the image compared to other IOLs with this technology.12 Decentration of some aspheric IOLs can lead to asymmetrical higher-order aberrations that adversely affect optical performance.12 Because of the natural capsular contraction after a cataract surgery, slight decentrations are common and expected.
A disadvantage of aspheric IOLs: the increased cost of the IOL. But, improved contrast sensitivity may make up for the difference.
Aspheric optics applied to IOLs can offer cataract surgery patients improved vision following surgery. That may be good news to cataract patients, whose ranks will increase by nearly 50% by 2020.
Dr. Karpecki has no financial interest in any products mentioned in this paper. However, he is a paid consultant to Bausch & Lomb.
1. Congdon N, OColmain B, Klaver CC, et al. Causes and prevalence of visual impairment among adults in the United States. Arch Ophthalmol 2004 Apr;122(4):477-85.
2. VisionConnection. Cost of Visual Impairment. www.visionconnection.org/Content/Research/EpidemiologyandStatistics/ Statistics/CostsofVisionImpairment/default.htm?cookie%5Ftest=1. Accessed September 19, 2005.
3. Marcos S, Barbero S, Jimenez-Alfaro I. Optical quality and depth-of-field of eyes implanted with spherical and aspheric intraocular lenses. J Refract Surg 2005 May-Jun;21(3):223-35.
4. Lua R. Exhibiting point aberrations in Gullstrands model of the eye via exact ray tracing. http://webusers.physics.umn.edu/~rlua/optics/project/gullstrand/node1.html. 2002 Dec 14. Accessed September 19, 2005.
5. Zhu L, Bartsch DU, Freeman WR, et al. Modeling human eye aberrations and their compensation for high-resolution retinal imaging. Optom Vis Sci 1998 Nov;75(11):827-39.
6. De Brabander, Chateau N, Bouchard F, Guidollet S. Contrast sensitivity with soft contact lenses compensated for spherical aberration in high ametropia. Optom Vis Sci 1998 Jan;75(1):37-43.
7. Thibos LN, Hong X, Bradley A, Cheng X. Statistical variation of aberration structure and image quality in a normal population of healthy eyes. J Opt Soc Am A Opt Image Sci Vis 2002 Dec;19(12):2329-48.
8. Dubbelman M, Van der Heijde GL. The shape of the aging human lens: curvature, equivalent refractive index and the lens paradox. Vision Res 2001 Jun;41(14):1867-77.
9. Christensen RE. The use of an aspheric lens for indirect ophthalmoscopy. Am J Ophthalmol 1959 Aug;48(2):256-7.
10. Werner W, Roth EH. Image properties of spherical as aspheric intraocular lenses. Klin Monatsbl Augenheilkd 1999 Apr;214(4):246-50.
11. Packer M, Fine IH, Hoffman RS, Piers PA. Improved functional vision with a modified prolate intraocular lens. J Cataract Refract Surg 2004 May;30(5):986-92.
12. Altmann GE, Nichamin LD, Lane SS, Pepose JS. Optical performance of 3 intraocular lens designs in the presence of decentration. J Cataract Refract Surg 2005 Mar;31(3):574-85.
