 |
The parents of an 11-month-old white female brought their daughter in for an evaluation. They had noted an abnormal white pupil reflex in the right eye in photographs for the past several months.
The parents also noted that the same eye appeared smaller than the left eye. They did not report any eye turn.
The patient was born following a full-term pregnancy and an uncomplicated delivery. She weighed 5 pounds, 11 ounces at delivery. There were no known health problems.
On examination, the patient had very poor fixation and following skills in her right eye, but she was able to easily fixate and follow with her left eye.
Also, she became visibly upset and angry when we placed a patch over her left eye, but not so when we patched the right eye. Hirschberg testing revealed orthophoria. There was a small afferent pupillary defect in the right eye.
Gross examination of the anterior segment showed that both globes appeared intact and well formed. However, there was obvious microphthalmia of the right eye (approximately 1-2mm) compared to the left.
Both corneas appeared normal; even the size of the right cornea appeared normal with respect to the size of the globe.
The anterior chamber was well formed and deep centrally in both eyes. The iris was flat without a mass. The lens was clear in both eyes, but a plaque of fibrous tissue was adherent to the back of the lens in the right eye.
On dilated fundus examination, significant fundus changes were found in the right eye and can be seen above. The fundus of the left eye appeared completely normal.
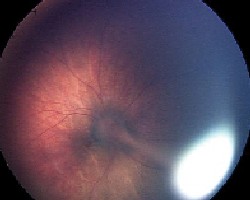 |
| Fundus photo of the right eye in an 11-month-old baby shows significant changes. A stalk of hyperplastic vitreous can be seen as it extends from the optic nerve and connects on the posterior surface of the lens. The details of the optic nerve are obscured. |
Take the Retina Quiz
1. Based on the patients history and external presentation, which of these can we immediately rule out?
a. Coats disease.
b. Persistent fetal vasculature,
or PFV.
c. Toxocara canis.
d. Retinoblastoma.
2. Which of the following is the primary etiology of this patients condition?
a. Failure of the primary vitreous to regress.
b. Infection from a nematode as a result of pica.
c. Congenital retinal telangiectasia.
d. Germline mutation.
3. What is the correct diagnosis for this patient?
a. Dominant familial exudative vitreoretinopathy.
b. Persistent fetal vasculature.
c. Toxocara canis.
d. Retinoblastoma.
4. Which is one of the most common complications of this condition if left untreated?
a. Exudative retinal detachment.
b. Dense cataract.
c. Angle-closure glaucoma.
d. Proliferative retinopathy.
5. How should this patient be managed?
a. Observation.
b. Pars plana vitrectomy and lensectomy.
c. Laser photocoagulation.
d. Both b and c.
Discussion
Retinoblastoma must be your first consideration when an infant presents with leukocoria. Fortunately, we can easily rule that out in this patient, as microphthalmia is not seen in retinoblastoma.
The microphthalmia we observed in this clinical setting is pretty diagnostic for persistent fetal vasculature (PFV).
PFV results from a failure of the primary vitreous and fetal vasculature to regress during normal fetal development. Some 90% of cases are unilateral.1
PFV originally was called persistent hyperplastic primary vitreous, or PHPV. However, the name PHPV only represented the more severe form of the condition and not the full spectrum of the disease, hence the name change.2
With the more severe form of PFV, a vascularized retrolental membrane can be seen behind the lens. The membrane runs posteriorly and connects at the optic nerve. Remnants of the fetal vasculature often can be seen within this membrane.
The membrane can act as a tether, in which it prevents the globe from growing in size as the child grows. This would explain why microphthalmia is universally seen with this condition.
The clinical spectrum of persistent fetal vasculature varies greatly, as remnants of the fetal vasculature and primary vitreous are frequently observed in patients as incidental findings.
As the disease has become better understood, three main forms of PFV have been described:
Anterior. Common findings such as persistent pupillary membranes (PPM) and Mittendorf dots represent milder forms of anterior PFV.
In more severe cases, a whitish or pinkish fibrovascular plaque may be present on the posterior surface of the lens; the plaque is often just nasal to the center of the lens.
Drawn-in ciliary processes can also be seen, depending on how large the plaque is. The crystalline lens is often clear, but a cataract will usually develop over time.
Posterior. Traction can result at the posterior pole as the stalk of hyperplastic vitreous pulls at the optic nerve and posterior pole. This can result in elevated vitreous membranes, retinal dysplasia and even retinal detachment.
Large retinal folds can also be present and radiate from the optic nerve anteriorly. Optic nerve hypoplasia can also be seen.
In milder forms of PFV, a persistent hyaloid artery and Bergmeister papilla can be seen but rarely affect acuity.
Combined. Most cases of persistent fetal vasculature have combined anterior and posterior features, with manifestations of both forms highly varied and even a high degree of overlap between the two forms. The purely posterior form occurs in only 10% to 20% of cases.1
The prognosis for PFV is poor, especially in the posterior and combined forms of the disease. Without treatment, eyes often progress to angle-closure glaucoma, blindness and finally phthisis bulbi.
Surgical intervention is recommended. This is not so much for visual recovery, but to prevent the above-mentioned complications from occurring.
Our patient has the combined form of PFV. A stalk of hyperplastic vitreous can be seen as it extends from the optic nerve and connects on the posterior surface of the lens. Note that the details of the optic nerve are obscured because of the hyaloid artery remnant.
The fibrous plaque on the posterior lens surface can also be visualized. Note also the clear view into the retina, indicating that the lens itself is clear.
Treatment and Follow-up
Our patient underwent both a vitrectomy and lensectomy without complications.
We fit her with a soft aphakic contact lens and initiated aggressive amblyopia therapy. Follow-up is ongoing.
Retina Quiz Answers: 1) d; 2) a; 3) b; 4) c; 5) b.
1. Murphree AL, Atchaneeyasakul L. Retinal detachments in infants. In: Ryan SJ, Schachat AP, Murphy RP, eds. Retina, Vol. III Surgical Retina. 3rd ed. St. Louis: Mosby, 2000:2505-7.
2. Goldberg MF. Persistent fetal vasculature (PFV): an integrated interpretation of signs and symptoms associated with persistent hyperplastic primary vitreous (PHPV). LIV Edward Jackson Memorial Lecture. Am J Ophthalmol 1997 Nov;124(5):587-626.
