 |
Acquired brain injury (ABI) can have severe visual consequences that can impact patients both in the short- and long-term. Under the umbrella heading of ABI, we include traumatic injury from car accidents and other blows to the head, often resulting in concussion, and nontraumatic injuries from stroke, surgery and neurological diseases such as ALS and MS. Depending on the severity of the injury, the patient’s symptoms and optometric findings may be variable. These symptoms can include blurred, doubled or lost vision, photophobia, reading difficulty, headache, balance issues and visual neglect/inattention. One study found an increased occurrence of exo deviations, oculomotor dysfunctions, vertical deviations, dry eye, blepharitis, optic nerve pathologies and visual field deficits in a population of adults who had sustained a brain injury.1
Photophobia is common following an ABI. It is not rare for patients to wear sunglasses both indoors and outside following their injury. We have even seen some patients present with sunglasses, a hat and a hoodie pulled over their heads. As with other symptoms related to ABI, the level of photophobia varies with the severity of the injury.
We can help these patients quite quickly and easily through the use of tints. This intervention can be added to a standard pair of glasses or prescribed as a fit-over on top of glasses or contact lenses. Researchers studied 51 concussed patients, 76% of whom complained of photophobia. Of those patients with photophobia, 85% were successfully treated with tints.2 In our experience at Southern College of Optometry (SCO) in the Vision Therapy & Rehabilitation Service, we can boast of similar treatment results. Here, we will present a case of successful treatment of ABI-related photophobia.
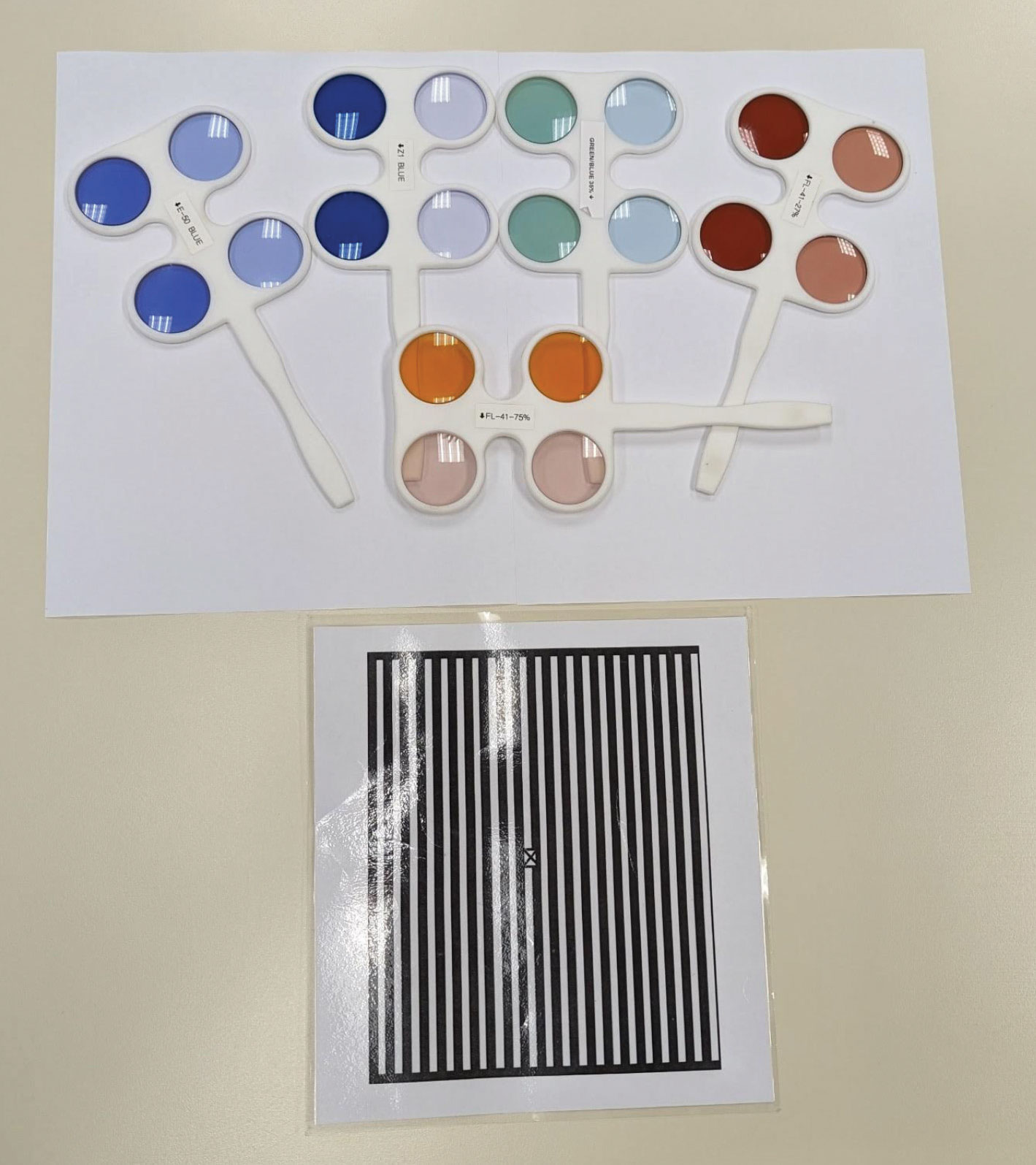 |
A variety of tints from the Chadwick Optical ABI flipper set and the Bowan grating card. Click image to enlarge. |
Case
A 19-year-old female college student presented with complaints of visual fatigue when reading, intermittent headaches and photophobia and increased blinking and refocusing with watering since her concussion 15 days prior. She also reported that her comprehension was worse and that she felt foggy since the event. While she was a college athlete, the concussion was sustained when a light fixture fell on her during a party.
The patient did not have a history of glasses wear, as was evident from her 20/20 acuities OD, OS and OU. Her confrontation fields, EOMs and pupils were all normal. Her BIVSS score was 65; a score above 31 is a red flag. Her cover test showed four exophoria at distance and 10 exophoria at near. A Maddox rod, along with a Thorington card at near, showed nine exophoria with a 0.5 left hyperphoria. Her NPC was receded at 7/9, 9/12 and 10/12 for break/recovery x three. Her near base-out vergence range was x/18/2, and her accommodative amplitudes were 5.00D OD and OS.
In working with concussion patients, the first goal is to make them more comfortable. Since small vertical misalignment can be a huge issue for ABI patients, we trialed a 0.5 base-down prism in front of the left eye, and the patient reported immediate improvement in the form of better clarity and focus.
Then, using the Bowan grating card—an alternating black and white card—we showed her five or six different tints from a premade, commercially available set from Chadwick Optical. Usually the response to a specific tint is immediately positive or negative, and this was indeed the case for this patient. She liked the most popular tint, the FL-41. The set has three saturation levels: 27%, 50% and 75%, and she appreciated the lightest tint. The prism and tint were made onto a base of plano lenses, and the patient was scheduled for a follow-up in four to six weeks to recheck her binocular status.
At the follow-up, the patient reported that her symptoms were significantly reduced and that she was wearing her glasses less and less. She was still visually fatigued, had occasional headaches and was having trouble focusing, but her fogginess and photophobia had abated. Her BIVSS score was now 42. Her binocular and accommodative testing continued to show a convergence insufficiency, and eye movement testing from RightEye showed poor fixation and saccades.
She was told to continue wearing her glasses full-time, and she was enrolled in vision therapy. While convergence insufficiency is a relatively easy condition to treat with therapy, the fact that it was secondary to a concussion in this case added an extra layer of complication. Even so, we expect her to make a full recovery.
 |
The patient wearing her FL-41 lenses. Click image to enlarge. |
Discussion
At SCO, we are lucky in that we have an amazing optical staff, and they have the most common tint formulas, including times for different saturations, down pat. Speak to your local optical and see if they can do the most common FL-41 as a starting point. The other option is to use an optical like Chadwick, which produces the ABI flipper set that we use most often to help patients select their preferred tint and saturation. There are six flippers in the set, with 12 different color/saturation combinations to choose from. Chadwick can make a pair of glasses with a specific prescription and tint in the frame of your choice. Fit-overs are the quickest way to get the tint on the patient. There are many commercial avenues to get FL-41 fit-overs in various saturations, and Chadwick has recently introduced fit-overs in several other colors as well.
Adding specialty tints for ABI to your practice not only sets you apart from other practitioners but also helps your patients recover from their injuries quicker. For young patients who play sports, concussions are unfortunately part of the game. Don’t assume that only football players are affected, as we have actually seen more concussions from soccer, basketball and volleyball. We have also not seen a gender or age preference with ABI. We have cared for stroke patients in their 30s; neurological disease can impact anyone. Consider adding a question about brain injury in your history evaluation. You will be shocked at how many people have ABI-related symptoms, especially photophobia, and how much of a difference you can make in their quality of life with even simple management methods.
Dr. Taub is a professor, chief of the Vision Therapy and Rehabilitation service and co-supervisor of the Vision Therapy and Pediatrics residency at Southern College of Optometry (SCO) in Memphis. He specializes in vision therapy, pediatrics and brain injury. Dr. Schnell is an associate professor at SCO and teaches courses on ocular motility and vision therapy. She works in the pediatric and vision therapy clinics and is co-supervisor of the Vision Therapy and Pediatrics residency. Her clinical interests include infant and toddler eye care, vision therapy, visual development and the treatment and management of special populations. They have no financial interests to disclose.
1. Suchoff IB, Kapoor N, Waxman R, Ference W. The occurrence of ocular and visual dysfunctions in an acquired brain-injured patient sample. J Am Optom Assoc. 1999;70(5):301-8. 2. Clark J, Hasselfeld K, Bigsby K, Divine J. Colored glasses to mitigate photophobia symptoms post-traumatic brain injury. J Athl Train. 2017;52(8):725-9. |
