 |
A 70-year-old male patient was referred for evaluation of lagophthalmos. The patient described a progressive and painful left facial droop with incomplete eyelid closure, facial numbness, hearing deficit and an inability to open the left half of his mouth. In addition, he reported difficulty eating over the course of four months and subsequent weight loss. His social histories were positive for chronic tobacco and alcohol use.
Best-corrected visual acuity measured 20/30 OU. Pupil testing was normal without afferent defect. Intraocular pressures were 15mm Hg OU. Extraocular motilities were full and smooth. Biomicroscopy revealed complete absence of left eyelid closure with a good Bell’s phenomenon. Anterior segment evaluation revealed severe keratopathy in the left eye secondary to chronic exposure. The lens showed 1+ nuclear sclerosis, and the vitreous was attached in both eyes. The optic nerves measured 0.20 OU, and the maculae were flat.
A physical evaluation of the motor functions of the seventh nerve revealed the inability to retract the left side of the face when asked to smile, close the left eye, wrinkle the forehead or open the left side of the mouth. Additional testing revealed normal function of cranial nerve five (CN-V), but reduced hearing in the left ear was consistent with cranial nerve eight (CN-VIII) dysfunction.
| Table 1. Motor Innervation of CN-VII: | |||
| Innervation | Function | Test | |
| Frontalis | Draws the scalp forward and wrinkles the forehead | Patient raises their eyebrows to wrinkle their forehead | |
| Orbicularis oculi | Eyelid closure | Attempt to open forcibly closed eyelids while noting any weakness between the two eyes | |
| Orbicularis oris | Closes the lips | Have the patient attempt to smile | |
| Buccinator | Puckers the lips | Have the patient attempt to puff the cheeks out | |
| Platysma | Wrinkles the surface of the skin in the neck, increases the diameter of the neck during rapid respiration, assists in depressing the angle of the mouth, improves venous flow | Have the patient attempt to contract the muscles of the neck | |
| Posterior belly of the digastric | Assists in opening the jaw | Have the patient attempt to open the mouth | |
| Muscles of the middle ear | Dampens sound to loud noises | Acoustic reflex impedance testing | |
Due to the patient’s history of chronic alcohol and tobacco use and the involvement of multiple cranial nerves (VII and VIII), emergent computed tomography (CT) of the head and neck was ordered. An immediate read by the radiologist revealed a large, infiltrative and enhancing, ill-defined mass centered on the ramus of the left mandible; additional CT of the brain was unremarkable.
To determine malignancy, a biopsy was taken of mucosal tissues from the left floor of the mouth and from the left retromolar trigone. Histopathology revealed poorly differentiated stage IV squamous cell carcinoma (SCC) of the left retromolar trigone. Ultimately, positron emission tomography (PET) revealed metastatic lung cancer. Both surgical and medical management of the tumor was considered; however, due to the progressive nature of the condition and its late staging, surgical resection would be unfavorable, and chemotherapy could not be performed secondary to poor nutritional status. From an ocular standpoint, the patient was prescribed viscous ophthalmic lubrication for use every few hours along with instructions on taping the outer one-third of the eyelid to reduce exposure; however, ultimately the patient was placed in palliative care and passed away one month after the initial diagnosis.
Discussion
CN-VII palsy is a relatively common neurologic condition. The rate of incidence in the general population is estimated to be 2% to 15%, with 75% to 90% attributed to idiopathic facial nerve paralysis (Bell’s palsy).1 The remaining causes of CN-VII palsy include: infection, inflammation, trauma, facial diplegia , iatrogenic and neoplasm (Table 1).1
The most common benign neoplastic cause of CN-VII palsy is facial nerve schwannoma and the most common malignant neoplasm is SCC.2 Neoplasm is responsible for a mere 5% of all cases of CN-VII dysfunction.3 In the United States, SCC of the head and neck represents 4% of all malignancies, but is responsible for more than 90% of all head and neck cancers.3 An epithelial-derived tumor, SCC is most commonly associated with alcohol and tobacco use, with significantly less incidence in those who neither smoke nor drink.4 The most common sites for SCC are: the floor of the mouth, tongue, soft palate, anterior tonsillar pillar and retromolar trigone, the last of which is aggressive and carries a poor prognosis.5
The facial nerve (FN) emerges from the brainstem between the pons and the medulla. It is predominantly responsible for the majority of all facial movement (Table 1) and, to a lesser extent, sensory function. It shares an anatomic locale with both major and minor salivary glands, mostly the parotid and submandibular glands. Disruption of the facial nerve at any location may result in sensory deprivation and partial or complete loss of facial function.
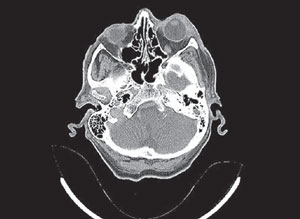 | |
| Large infiltrative and enhancing ill-defined mass of the left mandible and face, deviating the airway to the right. |
Presentations of FN weakness warrant comprehensive workup with special attention to the cranial nerves. Testing both upper and lower facial motor function helps differentiate between upper and lower motor neuron lesions; upper motor neuron (supranuclear) lesions result in contralateral facial weakness. Testing will show sparing of the upper face with paralysis of the contralateral lower face. For example, a patient with a right CN-VII palsy from a left upper motor neuron lesion will present with lower FN weakness on the right side with sparing of the frontalis and orbicularis oculi muscles. The patient will be able to furrow their forehead and close their eyelid, but will show weakness when asked to puff the cheeks, smile, open their mouth and pucker their lips. A lower motor lesion, as seen in our patient, affects the main trunk of the facial nerve and causes ipsilateral weakness in both upper and lower facial regions. FN paralysis involving a history of pain, multiple CN involvement and recalcitrant behavior should be investigated with MRI or CT of the head and neck to exclude tumor, demyelination and stroke, and laboratory testing to exclude infection and inflammation.
The ocular management of CN-VII paresis may include both medical and surgical therapies. If the patient cannot close their eye, lubrication of the cornea is necessary to prevent secondary-exposure keratitis and subsequent corneal ulceration. The mainstays of therapy are nonpreserved artificial tears used frequently while awake and ophthalmic ointments at bedtime. If significant lagophthalmos exists, the palpebral aperture can be narrowed by applying transparent, medical-grade tape to the lateral aspect of the lower eyelid, then directing the tape upward and laterally, securing it to the orbital rim; this will act as a temporary tarsorrhaphy.
External eyelid prostheses can also be used as short-and long-term treatment for patients with temporary facial paralysis and as a trial before implantation of eyelid gold weights. Moisture chamber goggles and punctal occlusion can also provide additional moisture. In the presence of severe keratopathy or corneal ulceration, a bandage contact lens and amniotic membrane may be helpful.6,7 In the event of persistent corneal decompensation, treatment options may include complete or partial tarsorrhaphy, gold-weight insertion in the affected upper eyelid to induce a ptosis and surgical intervention with a lateral canthal strengthening procedure (canthoplasty) to repair ectropion.8
This case represents an atypical, low prevelance cause of facial nerve paralysis; however, a careful history, review of systems, physical examination and proper neuroimaging increase the odds of a timely and accurate diagnosis.
1. Finsterer J. Management of peripheral facial nerve palsy. Eur Arch Otorhinolaryngol. 2008;265(7):743-52.2. Gross BC, Carlson ML, Moore EJ, et al. The intraparotid facial nerve schwannoma: a diagnostic and management conundrum. Am J Otolaryngol. 2012;33(5):497-504.
3. Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer J Clin. 2008;58(2):71-96.
4. National Cancer Institute. Alcohol and Cancer Risk. Accessed November 2015. www.cancer.gov/about-cancer/causes-prevention/risk/alcohol/alcohol-fact-sheet.
5. Hao SP, Tsang NM, Chang KP, et al. Treatment of squamous cell carcinoma of the retromolar trigone. Laryngoscope. 2006;116(6):916-20.
6. Yildiz EH, Nurozler AB, Ozkan Aksoy N, et al. Amniotic membrane transplantation: indications and results. Eur J Ophthalmol. 2008;18(5):685-90.
7. Suri K, Kosker M, Raber IM, et al. Sutureless amniotic membrane Prokera for ocular surface disorders: short-term results. Eye Contact Lens. 2013;39(5):341-7.
8. Kartush JM, Linstrom CJ, McCann PM, Graham MD. Early gold weight eyelid implantation for facial paralysis. Otolaryngol Head Neck Surg. 1990;103(6):1016-23.
