 |
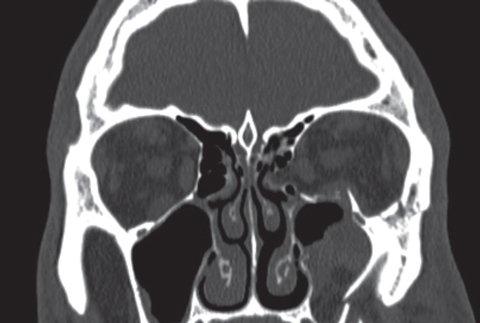
The majority of ocular injuries found in cases of intimate partner violence were orbital fractures, as seen here, followed by contusion of the eyelid and periocular eyelid and injury of the eye and orbit. Photo: Sean Dempsey, OD. Click image to enlarge. |
Even with ongoing prevention and awareness initiatives, intimate partner violence continues to be a widespread cause of mortality and disability internationally. Not only is this type of violence a commonplace occurrence in the United States, it also has serious long-term consequences for survivors’ health. For instance, trauma inflicted to the eyes and visual pathway has demonstrated sight-threatening consequences like glaucoma, retinal detachment, retinal hemorrhage, ruptured globes and orbital fractures.1 Eyecare practitioners can play a crucial role in the detection and prevention of these circumstantial injuries.
A recent study published in JAMA Ophthalmology helped identify important risk factors of ocular injuries in survivors of intimate partner violence. A 2017 to 2019 analysis of the National Trauma Data Bank—the largest US hospitalized trauma case database with submissions from more than 900 facilities in the country—illustrated that almost two-thirds of ocular trauma survivors were female, roughly one-third had Medicaid insurance and approximately one-half were Caucasian. Nevertheless, intimate partner violence is heavily underreported across all ethnic and racial groups, and the researchers noted that it has been disproportionately underreported in ethnic minorities.1
In the United States, the CDC defines intimate partner violence as “physical violence, sexual violence, stalking or psychological aggression by a former or current intimate partner, whether or not the partner is a spouse.” This is distinct from domestic violence, which generally refers to violence occurring between individuals living together in a single location who are not necessarily significant others.
Reporting on the epidemiologic characteristics, patterns and prevalence of patients seeking hospital care for eye injuries due to intimate partner violence, the research team used the National Trauma Data Bank. Ocular injuries and adult trauma survivors from intimate partner violence were identified through the ICD-10-CM codes. Between 2017 and 2019, 345,733 (67.9%) ocular injuries were sustained by males, and 163,150 (32.1%) were sustained by females.
However, when observing ocular injuries specifically related to intimate partner violence, 62.3% of cases involved female survivors. A total of 2,598 of the recorded ocular injuries were associated with intimate partner violence. Patients had a mean age of 45.2, and most in the population sample (46%) were between 18 and 39 years old. The race and ethnicity distribution was as follows: 24.2% Black, 11.4% Hispanic, 52.3% Caucasian, 8.8% other and 3.3% missing. Insurance statuses were Medicaid (32.6%), Medicare (20.2%), private insurance (20.2%) and self-pay (18.8%). Black patients were most likely to have Medicaid (OR: 1.64), Hispanic patients were most likely to self-pay (OR: 1.96) and Caucasian patients were most likely to use Medicare (OR: 2.94). High-risk behaviors, such as harmful alcohol and drug use, were more frequent among survivors of interpersonal violence. Women had greater odds of testing positive during alcohol screening (OR: 1.42).1
Ocular trauma in the United States due to intimate partner violence was more prevalent among individuals between the ages of 18 and 39. Women were disproportionately affected by intimate partner violence-related ocular trauma. Key risk factors included the following social determinants of health: sex, substance abuse, race and ethnicity, age, social support and socioeconomic resources. Orbital fractures, which are vision-threatening, were the most common intimate partner violence-related ocular injury at 37.1% of cases. This was followed by contusion of the eyelid and periocular eyelid (25.8%) and injury of the eye and orbit (19.9%).
“Our results suggest that specific culturally sensitive screening guidelines may be needed for suspected intimate partner violence-related ocular trauma to help identify trauma survivors from vulnerable populations,” the study authors wrote in their paper. “Furthermore, investigations should be conducted to accurately identify the appropriate screening interventions toward ethnic minority groups for ocular trauma related to this situation.”1
A commentary, also published in JAMA Ophthalmology, supported the study’s suggestion that eyecare providers may play an important role, beyond treatment of the injury, in helping identify intimate partner violence and enable prevention strategies.2
“With 45% of injuries involving the eye that are related to intimate partner violence, the practitioner should have a high index of suspicion for this scenario in female patients with orbital fractures and/or ocular injuries,” the authors wrote.
The commentary proposed that arming eyecare providers with better access to violence-related screening tools would likely reduce ocular morbidity.
“Data on the distinctly different profile of these kinds of ocular injuries—with those at highest risk for orbital fractures and/or contusions being female individuals older than 40 years, with most injuries taking place in the home—may help guide the development of programs to effectively identify survivors of intimate partner violence,” the commentary authors concluded.
| 1. Alik M, Malik M, Ashrafi R, Wu AY. Epidemiologic pattern and injury mechanism of intimate partner violence–related ocular trauma in the US. JAMA Ophthalmol. March 30, 2023. [Epub ahead of print]. 2. Hoskin AK, Watson SL. Intimate partner violence and the role of ophthalmology. JAMA Ophthalmol. March 30, 2023. [Epub ahead of print]. |
