 |
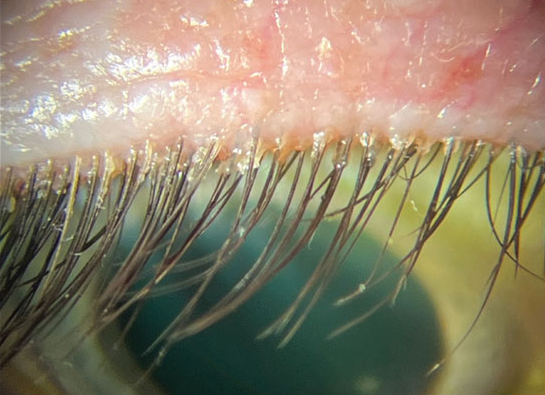
| The proposed treatment algorithm for Demodex blepharitis begins with removal of cylindrical dandruff using lid hygiene techniques and products, then tea tree oil (TTO) 5% BID. After four to six weeks of this regimen, the patient is to be evaluated again. If there’s little to no clinical improvement, consider one of these four options to escalate therapy: increase frequency of lid cleaning; administer TTO at a concentration of 50% in the office; add oral therapy; recommend intense pulsed light therapy. Photo: Cecelia Koetting, OD. Click image to enlarge. |
Recently, a Delphi study conducted by the Demodex Expert Panel on Treatment and Eyelid Health (DEPTH) in the United States has reported on signs, symptoms, diagnosis and management for Demodex blepharitis. A different study, published in Contact Lens and Anterior Eye, took a similar approach to arrive at best practice recommendations based on experts working in the United Kingdom. This UK study developed a diagnostic algorithm along with management guidelines that can be used in optometric practice and education for clinical investigation of Demodex blepharitis. Tea tree oil and Blephademodex eyelid wipes (Thea Pharmaceuticals) were considered the most appropriate first-line treatment option for Demodex.
The Delphi technique is a multi-stage process, consisting of different iterations or rounds among a group of professionals/informed individuals or experts. The expert panel comprised two ophthalmologists, eight optometrists and one contact lens optician all working in the UK. Most experts did not follow any guidelines while examining the eyelids. This is likely because Demodex blepharitis does not have any standardized practice guidelines. The rest of the experts followed using tea tree oil as per the recommendations from the DEWS-II Management and Therapy Report and the College of Optometrists’ Clinical Management Guidelines.
The expert panel reached the consensus that Demodex blepharitis is an under-diagnosed condition in routine clinical practice, is a significant cause for ocular discomfort and is a potential cause for an unstable tear film. The expert panel also recommended eye care practitioners to look for Demodex mites in routine clinical practice. They perceived Demodex to be more prevalent in elderly individuals (median: 60 years old).
The panel agreed that signs and symptoms correlate well in symptomatic patients. Lid margin itch, grittiness and foreign body sensation were the most associated symptoms, while visible Demodex mites, presence of cylindrical dandruff and anterior blepharitis not responding to treatment, were the most associated signs.
“A consensus was also achieved that signs and symptoms do not correlate in asymptomatic patients,” the authors noted in their paper. “While Demodex is present in all of the individuals, it does not necessarily cause a disease since Demodex is considered to contribute to the normal ecology of the eyelid.”
The study highlighted that meibomian gland disease (MGD) and dry eye disease (DED) may either co-exist with Demodex blepharitis, or Demodex could lead to (or aggravate) already present MGD/DED. Therefore, due to coexistence/overlap in signs and symptoms, efforts should be made to differentially diagnose these ocular surface diseases.
Six of the panel recommended commencing first-line treatment twice-a-day. However, the whole panel reached a consensus with a treatment duration of four to six weeks. They also suggested reviewing the patients between two and six weeks after commencing treatment. If the first-line treatment is not effective, the expert panel also reached a consensus to switch to a second-line treatment within two to six weeks.
“The second-line treatment could be more rigorous in providing symptomatic relief and may include increased frequency of lid cleaning, in-practice treatment using high concentration of tea tree oil, intense pulse light, eyelid debridement, oral drugs (i.e., azithromycin and doxycycline) or additional pharmacological treatment, such as topical antibiotics,” the authors wrote.
“We suggest that the diagnostic and treatment algorithms developed in this study could be used by eye care practitioners in the UK and beyond in their clinical practices to effectively evaluate and manage Demodex blepharitis,” the study concluded. “The authors acknowledge that high quality research in this area is limited, and future research could bring new insights and interesting developments on the subject.”
Sharma N, Martin E, Pearce EI, Hagan S. A Delphi approach to establishing consensus on best practice for the diagnosis and treatment of Demodex blepharitis. Cont Lens Anterior Eye. November 8, 2023. [Epub ahead of print]. |
