 |
Q:
Is combining corneal crosslinking (CXL) and Intacs for keratoconus a viable option? What does it involve? What requirements do patients have to meet for candidacy? What other considerations need to be taken into account?
A:
Surgical treatment of keratoconus has substantially advanced over the past two decades, according to Brian Chou, OD, of San Diego. In July 2004, the FDA granted Humanitarian Device Exemption approval to Intacs (Addition Technology) for keratoconus. Then, in April 2016, the FDA granted approval for the KXL crosslinking system by Avedro (since acquired by Glaukos) for progressive keratoconus.
CXL decreases the progression of keratoconus and incrementally flattens the topographical shape of the cornea. Intracorneal ring segments (ICRS) for keratoconus, i.e., Intacs or Ferrara rings (Mediphacos), can smooth out and flatten the corneal surface.
 |
|
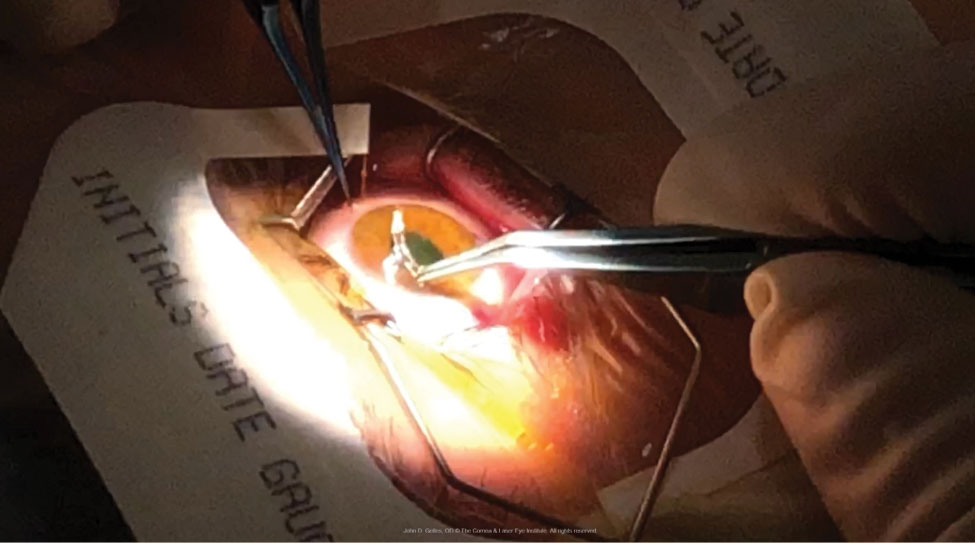
An ICRS is placed into an intrastromal channel immediately after undergoing CXL. Note the riboflavin-induced yellow hue of the cornea. Photo: John Gelles, OD. Click image to enlarge. |
A Combined Effect
The safety and efficacy of CXL and Intacs, performed both concurrently and sequentially, was recently evaluated in 198 patients of the Cornea and Laser Eye Institute (CLEI) in Teaneck, NJ.1 Enrolled keratoconus participants were 21 years or older. Excluded patients had a corneal thickness less than 350µm at the thinnest point or other conditions predisposing them to surgical complications.
John Gelles, OD, of CLEI, explains that, “in a concurrent treatment, the patient will first undergo an intrastromal ring dissection with a femtosecond laser, followed by CXL and finally the implantation of the ICRS.” By contrast, in a sequential procedure CXL is performed first and ICRS happens weeks to months after. “In our randomized prospective clinical trial, we compared concurrent (same-day CXL and ICRS) with sequential (three months between CXL and ICRS) surgery.”
The research team found that outcomes between the two were equivalent, the combined procedure was safe and there was no comparative increased risk associated with one or the other. Dr. Gelles notes that a well-placed, single segment ICRS implant provided the largest curvature reduction and visual improvement.
While adjunctive CXL and Intacs offers more flattening of the corneal distortion than either procedure alone, Dr. Chou says all patients undergoing combined surgery can expect to wear rigid-surface contact lenses afterwards for maximal vision. “No surgery at present can make the distorted cornea in keratoconus as smooth as the surface of a rigid-surface contact lens,” he says. “However, combined CXL and Intacs may provide carefully selected keratoconus patients—including those with milder distortion and myopia—with sufficient vision with glasses or soft contact lenses.”
Patient Selection
These patients must understand that undergoing CXL or Intacs may cause them to lose eligibility for necessary contact lenses under a vision plan, notes Dr. Chou. For example, one criterion of EyeMed Vision Care for “moderate/severe keratoconus” is a topographical steep keratometry value of 53.00D or greater.2 “If CXL and/or Intacs causes the patient’s keratometry value to fall below 53.00D but they end up as visually dependent on scleral lenses as beforehand, the EyeMed patient must bear the full cost of scleral contact lenses and prescribing services, which can exceed $3,000 each year,” Dr. Chou says. To set realistic expectations, Dr. Chou recommends optometrists discuss this with patients preoperatively so they have the necessary information to decide which course of action makes the most sense for them moving forward.
Take-home Message
Combining CXL and Intacs is a suitable defensive play for select cases of keratoconus. CXL can prevent disease progression, while Intacs can provide functional vision with glasses or soft contact lenses. However, the offensive play to bring out maximal vision remains rigid contact lens optics, most commonly with scleral contact lenses.
Dr. Shovlin, a senior optometrist at Northeastern Eye Institute in Scranton, PA, is a fellow and past president of the American Academy of Optometry and a clinical editor of Review of Optometry and Review of Cornea & Contact Lenses. He consults for Kala, Aerie, AbbVie, Novartis, Hubble and Bausch + Lomb and is on the medical advisory panel for Lentechs.
|
1. Hersh PS, Issa R, Greenstein SA. Corneal crosslinking and intracorneal ring segments for keratoconus: a randomized study of concurrent versus sequential surgery. J Cataract Refract Surg. 2019;45(6):830-9. 2. Chou B. New tools to tame keratoconus. Rev Optom. 2019;156(4):42-8. |
