 |
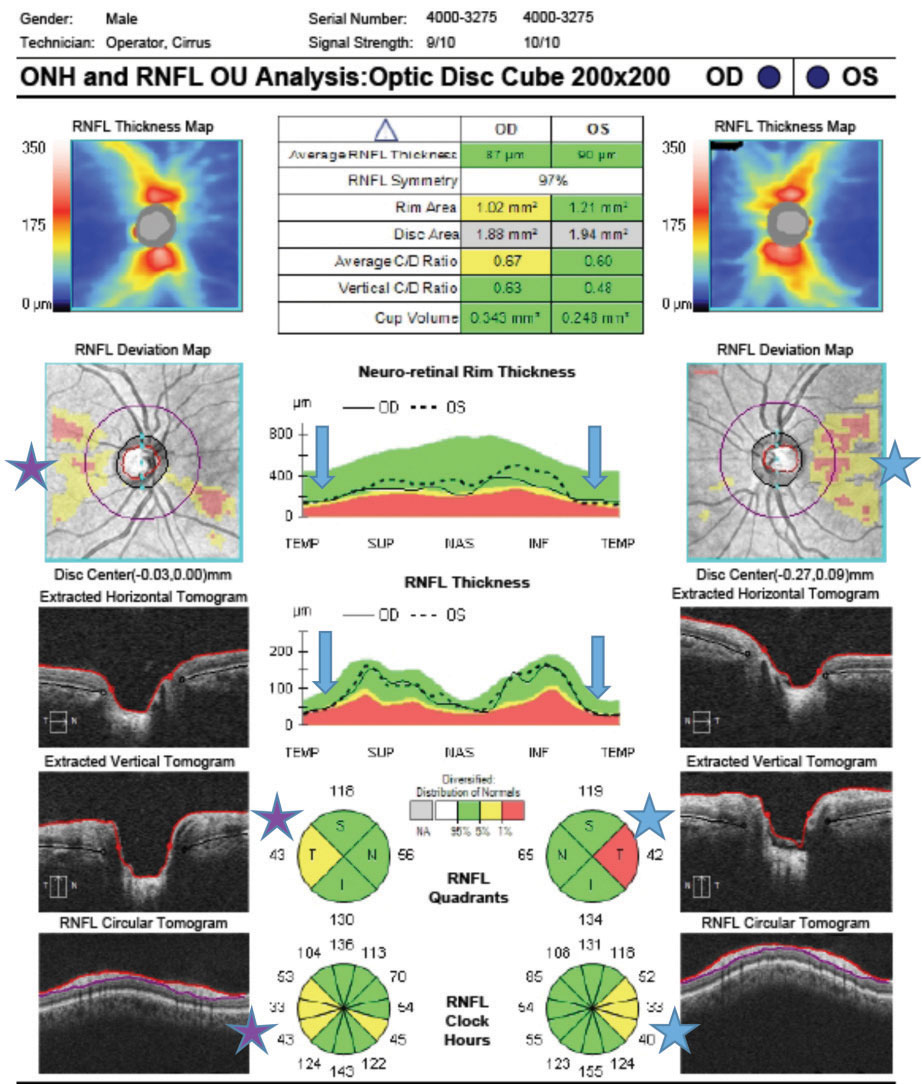
There was a significantly less negative mean RNFL slope globally and in three of the six sectors when baseline categories was progressively worse (within normal limits through outside normal limits). In contrast, this was true for only one sector with MRW change. Photo: Jarett Mazzarella, OD, and Justin Cole, OD. Click image to enlarge. |
Optic nerve minimum rim width (MRW) and peripapillary retinal nerve fiber layer (RNFL) thickness measurements are two key OCT measurements used in diagnosing glaucoma and detecting its progression. However, because of the limitations imposed by the so-called “floor effect”—the point at which glaucomatous damage becomes so pronounced that further progression cannot be measured by OCT—it is unclear how reliable these measures are, especially in patients with atypical baseline characteristics. Clinicians also find it hard to determine whether there is a differential floor effect of MRW and RNFL thickness with respect to measuring change.
To determine whether more severe baseline damage impedes measurement of MRW and peripapillary RNFL thickness change in glaucoma patients because of a floor effect, researchers based in Halifax, Nova Scotia quantified the impact of global and sectoral baseline MRW and RNFL thickness, and the corresponding baseline categories, on the ability to detect future glaucomatous change. Their study demonstrated that statistically significant changes in global and sectoral MRW and RNFL thickness were detected across all baseline classifications; however, there was tendency for less change with increasing baseline damage.
The study included a total of 97 patients with glaucoma (median age, 70.3 years) and 42 healthy subjects (median age, 64.8 years) were followed for a median of 6.9 years and 7.0 years, respectively. The follow-up period for each participant was divided into two equal halves (first and second periods) to determine whether there was attenuation of MRW and RNFL thickness change with follow-up time. The median mean deviation of visual field test for the glaucoma patients was -4.30dB (range: -20.68dB to 1.37dB).
RNFL thickness slopes, but not MRW slopes, were significantly more positive (less change) in the second period compared with the first among glaucoma patients. There were also no differences in either MRW or RNFL thickness slopes in the first and second periods in healthy subjects. Significant change of MRW was detected in almost 75% of glaucoma patients who had a global baseline classification that was outside normal limits. For RNFL thickness, the figure was slightly less. There was an attenuation in the rate of change that was more evident with RNFL thickness compared with MRW, suggesting significant differences in tissue response to axonal loss at the level of the optic nerve head and peripapillary retina.
“From a practical perspective, these findings indicate that OCT imaging remains beneficial despite MRW and RNFL thickness baselines that are below the first percentile of normative values,” the study authors wrote in their paper, which was published in Ophthalmology.
Most patients had mild to moderate glaucomatous damage, with only a small number of patients with advanced glaucoma. The researchers suggested that a study population with more advanced damage may have demonstrated a flatter floor effect.
“Significant MRW and RNFL thickness change can be detected for all baseline categories,” they concluded.
Tomita R, Rawlyk B, Sharpe GP, et al. Progressive changes in the neuroretinal rim and retinal nerve fiber layer in glaucoma: impact of baseline values and floor effects. Ophthalmology. January 1, 2024. [Epub ahead of print]. |
