 |
History
A 57-year-old Black male reported to the office with a chief complaint of a swollen eyelid that had been bothering him for a day. He explained that he had gone to sleep feeling normal, but when he woke up, he had a swollen lid. His systemic and ocular histories were unremarkable and he denied exposure to chemicals or knowing of any allergies.
Diagnostic Data
His best-corrected entering visual acuities were 20/20 OU at distance and near. Extraocular muscles and confrontation fields were normal and he showed no evidence of afferent pupillary defect. The biomicroscopic examination of the anterior segment was normal and the external examination is demonstrated in the photograph (Figure 1). Goldmann applanation tonometry measured 15mm Hg OU.
The dilated fundus findings were normal peripherally and centrally with normal nerves and maculae.
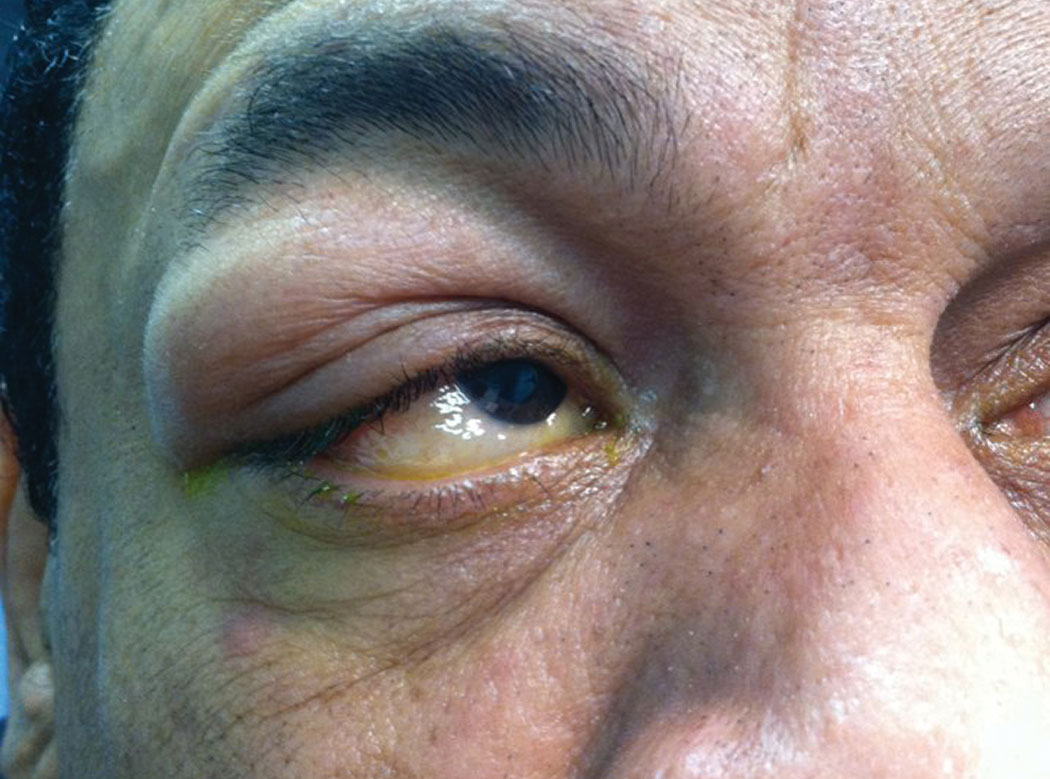 |
| Fig. 1. This patient went to sleep feeling fine, but something went bump in the night—his eyelid. Can you identify what caused this and how he should be treated? Click image to enlarge. |
Discussion
Additional studies included palpation of the eyelids and examination for unusual focal swelling.
The diagnosis in this issue is Type I anaphylactic allergic dermatitis secondary to a presumed bite from a bed mite.1-5 The phylum Arthropoda includes arachnids and insects.1,2 Although their bites typically cause only local reactions, some species can inject toxic venom or transmit disease.1 The allergic reaction is based in the human Type I, III, and IV immune response.3 Bed bugs have the ability to impart mild to severe cutaneous vasculitic reactions.3,5 Bed bug salivary extract (SGE) is responsible for inducing inflammatory reactions via the production of several potent chemokines and cytokines from macrophages.3 Chemokines induced by SGE include those known to recruit eosinophils (eotaxin), attract neutrophils [interleukin (IL)-8] or induce their survival and proliferation (granulocyte colony-stimulating factor).3 Cytokines involved in cell-mediated immunity, including IL-7, IL-10 and IL-12, are also induced.3 The saliva of bed bugs contains protein and non-protein molecules that have pleotropic effects on macrophages, orchestrating the prominent immune response seen in the epidermis after bed bug bites.3
Most bites resolve uneventfully without aggressive therapy and require only wound care and minor epithelial debridement. Scratching the itchy, affected area can cause further injury and seed the region with bacteria producing secondary infection.4 Bites from fleas, bed bugs and mites can treated with cold compresses, oral antihistamines and in the case of severe reactions medium potency topical steroidal creams and oral prednisone.5 Topical over-the-counter antibiotic ointments and anti-itch creams/sprays can add prophylactic anti-infective coverage while reducing discomfort.
This patient’s treatment was approached in a step-wise fashion using cold compresses, oral anti-histamines and over-the-counter topical anti-itch cream. The condition resolved in entirely in 48 hours. If this had not worked, a steroid pack would have been considered depending on the level of healing.
|
