 |  |
Foveoschisis due to myopic traction maculopathy is recognized as the splitting of the inner retinal layers at the macula in patients with high myopia and posterior staphyloma. The pathogenesis is thought to be multifactorial, involving anterior traction, rigidity of the internal limiting membrane (ILM) and progression of the posterior staphyloma. Patients tend to be asymptomatic initially, but central vision loss slowly progresses over time with the formation of foveal detachment and/or macular hole.1 They are often unaware they have foveoschisis due the condition’s slowly progressive nature, but this gives indication for surgical intervention.
OCT is the main diagnostic tool for confirming the presence of foveoschisis, as it focuses on the presence of epiretinal membrane, retinal thickening, vitreomacular traction, separation of neurosensory retinal tissue in two or more layers, retinal detachment lamellar or full-thickness macular holes.1,2
Once OCT confirms foveoschisis, it’s time to plan for surgery—pars plana vitrectomy with membrane peel.
 |
|
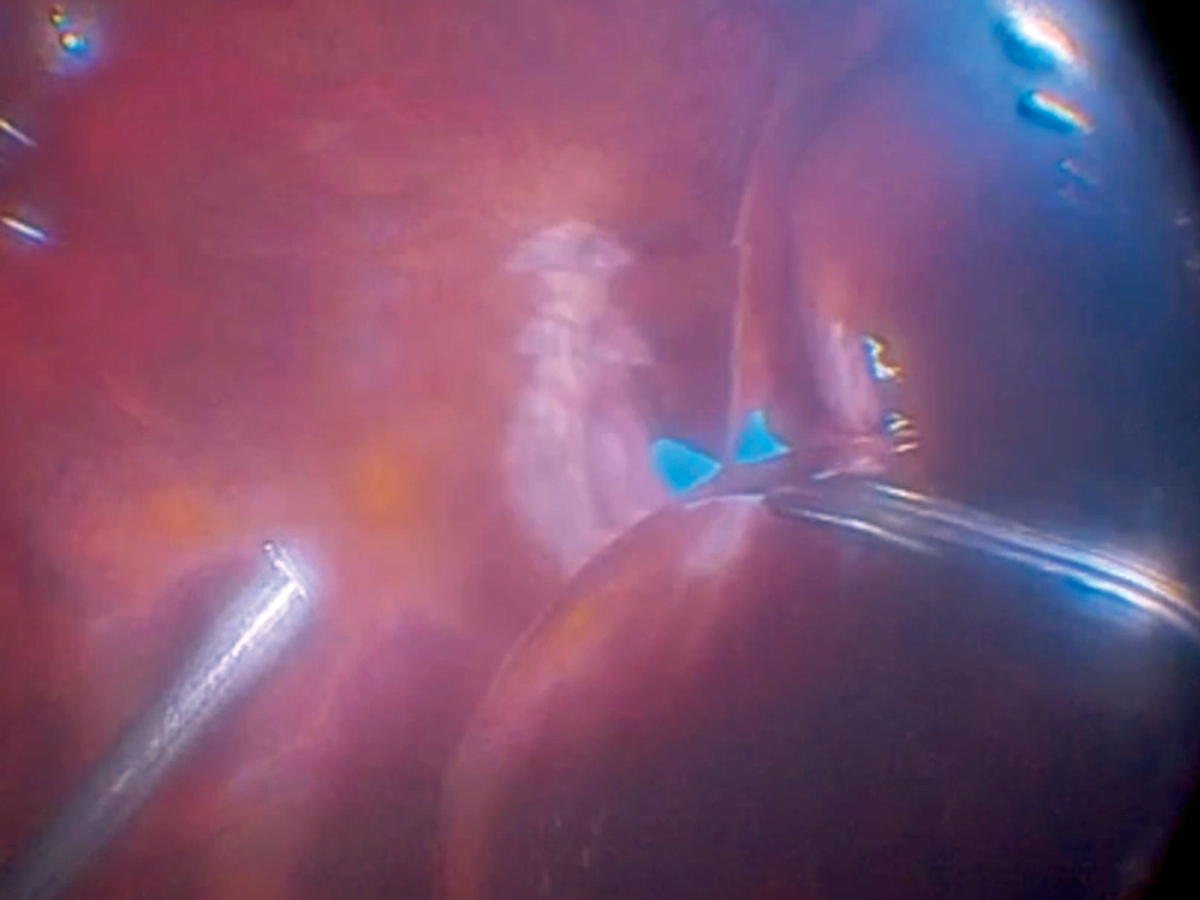
An ILM peel in an eye presenting with foveoschisis and poster staphyloma. Click image to enlarge. Photo: Alan Franklin, MD |
The Procedure
In vitrectomy with membrane peel procedures, the instruments are usually inserted 4mm behind the limbus.3 The surgery, typically performed in an outpatient center, takes about 45 minutes. It is conducted under local anesthesia with very small incision ports that do not require suturing.3 Visual recovery varies from patient to patient, but can be dramatic the next day.3
Pre-retinal tissue is removed from the superficial inner retina with a 25-gauge sharkskin forceps. The procedure demonstrates a large diameter peel that borders the edge of the staphyloma. Brilliant blue or indocyanine green dye is used to stain the ILM and enhance structural identification. Following the membrane peel, a diluted gas tamponade is put in place for structural integrity.
In the video, which can be viewed online, the surgeon explains how unforgiving and delicate the retina is underneath the membrane, and stresses the importance of gentle removal of the tissue to avoid iatrogenic tears or holes. These are typically some of the more challenging cases, due to the thin retinal tissue in highly myopic patients.
Treatment
Pars plana vitrectomy along with ILM peeling has shown good results in relieving traction on the macula and reducing recurrence by removing the scaffold for the proliferation of glial cells.1 Peeling the ILM can cause iatrogenic macular holes, which may lead some surgeons to prefer another means of treatment.4 It is important that the surgeon identifies the directionality of the tractional force on the retina, taking into account both forces tangential or perpendicular to the plane of the retina and choosing a treatment option that mitigates that force.1
The most common surgical complications include infection (roughly one in 1,000 procedures), retinal detachment (roughly one in 100 procedures), cataract progression in phakic eyes, bleeding and diplopia.3
The goal of surgery is to relieve abnormal traction of the vitreous and to tamponade the posterior retina to the protruding staphyloma. Currently, this is the most favorable surgical treatment, but new techniques and approaches will continue to evolve.
Dr. Martin is an ocular disease resident at Dell Laser Consultants in Austin, TX. He has no financial interests to disclose.
1. Raizada K, Sahu J. Myopic Foveoschisis. Updated September 24, 2022. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Accessed November 16, 2022. 2. Sayanagi K, Morimoto Y, Ikuno Y, Tano Y. Spectral-domain optical coherence tomographic findings in myopic foveoschisis. Retina. 2010;30(4):623-8. 3. Cunningham DN, Whitley W. Vitrectomy with membrane peel. Rev Optom. 2013;150(1):96. 4. Kuhn F. Internal limiting membrane removal for macular detachment in highly myopic eyes. Am J Ophthalmol. 2003;135(4):547-9. |
