 |
Tobacco use kills approximately 440,000 Americans each year, and one in every five US deaths is the result of smoking.1,2 While the majority of these patients are killed by smoking cigarettes, tobacco use in other forms contributes to worldwide morbidity and mortality.1-3 Smoked forms of tobacco other than cigarettes, including cigars, traditional pipes and water pipes, erroneously are often perceived as much less hazardous than cigarettes.3
New nicotine delivery systems not directly reliant on tobacco, such as electronic cigarettes, are also becoming increasingly popular, especially among teens and adolescents.
Smoking and the Eye
Several ocular conditions are directly or indirectly related to smoking. For one, smoking is an established risk factor for cataract. Cessation of smoking appears to decrease the risk of cataract, but cataract risk among former smokers persists for decades. Formation of free radicals and lower levels of circulating antioxidants may initiate the ocular pathogenesis by oxidative stress. There is evidence of a dose-response effect of smoking on ocular morbidity.4
Other associated ocular conditions include age-related macular degeneration, dry eye disease, diabetic retinopathy, ocular ischemic syndrome, retinal vascular occlusions, anterior ischemic optic neuropathy, thyroid eye disease and metastatic carcinoma of the uvea.5,6
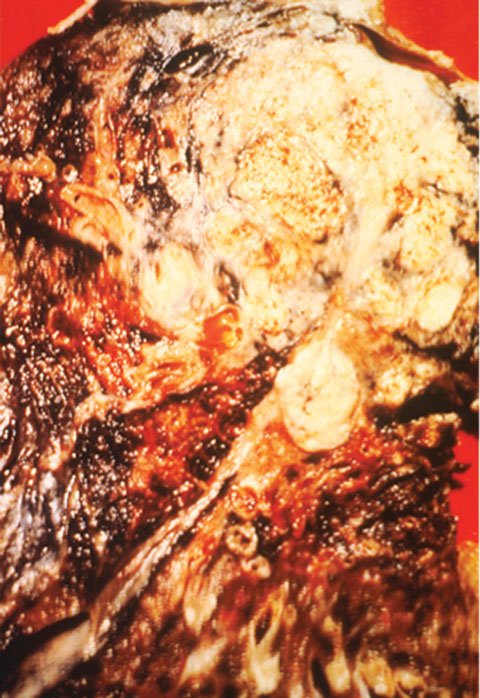 |
| Cross-section of a lung. The black areas indicate the patient was a smoker, and the white area is cancer. Image: National Cancer Institute |
Everything But Cigarettes
Because smoking can have such a profound effect on the eye, optometrists should be aware of the various methods of smoking and be prepared to educate patients on their associated risks. For more information on cigarettes and cigars, see part one, available at www.reviewofoptometry.com/article/smoke-or-vapor-gets-in-your-eyes-part-one.
Traditional pipes are usually composed of a bowl, in which the tobacco is placed for burning, attached to a stem through which the smoke is drawn. The tobacco used in pipes may sometimes be flavored.5 One study reported that the total particulate matter extracted from pipes was up to 44% more mutagenic per unit of nicotine, relative to cigarette smoke.7 As with cigars, pipe use is associated with cancers of the mouth, nose and upper airway.7
Water pipes—known in various regions by names such as shisha, hookah and narghile—typically employ indirect heating of tobacco (often via charcoal). The smoke generated is passed through a chamber containing water before reaching the user through a hose. The proliferation of water pipe cafes may be due, in part, to the introduction of flavored tobacco preparations.3,8 Water pipe use appears to be especially popular among university students, many of whom believe it is less hazardous than cigarette smoking.
However, the water in the pipe does not act as a real filter. During a 20- to 80-minute hookah session, users may smoke the equivalent of 100 or more cigarettes.9 In addition, the use of charcoal as a heating source generates large amounts of carbon monoxide and polycyclic aromatic hydrocarbons.3,6,7 Although the literature on the health effects of water pipe use isn’t robust, what little is available indicates water pipe use is associated with cancer, heart disease, lung malfunction, infectious diseases and reproductive side effects.8
Nicotine delivery systems not directly reliant on tobacco, such as electronic nicotine delivery systems (ENDS) known as e-cigarettes, are becoming increasingly popular. These devices work by vaporizing a solution containing nicotine dissolved with flavorants in a carrier medium (usually propylene glycol).3 The nicotine used in e-cigarettes is most frequently derived from tobacco. Companies promote ENDS with claims that they have reduced health risk compared with tobacco use and can be used in situations where smoking is prohibited.3,10
Of major concern is their widespread use by teens and adolescents. In addition, studies reveal many e-cigarette smokers are dual users (they also smoke another form of tobacco). The FDA has not found e-cigarettes safe and effective in helping smokers quit.3,10,11
With respect to health hazards, data on ENDS are lacking. Nicotine delivered by vapor with few known toxicants should theoretically carry relatively low risks, particularly when compared with cigarettes. The limited data available suggests these products are not likely to approach the health hazards of cigarettes. However, significant concerns exist about the purity of ingredients used, device functionality and quality control, the ease with which devices can be modified by users and the general lack of oversight in manufacturing and marketing.11
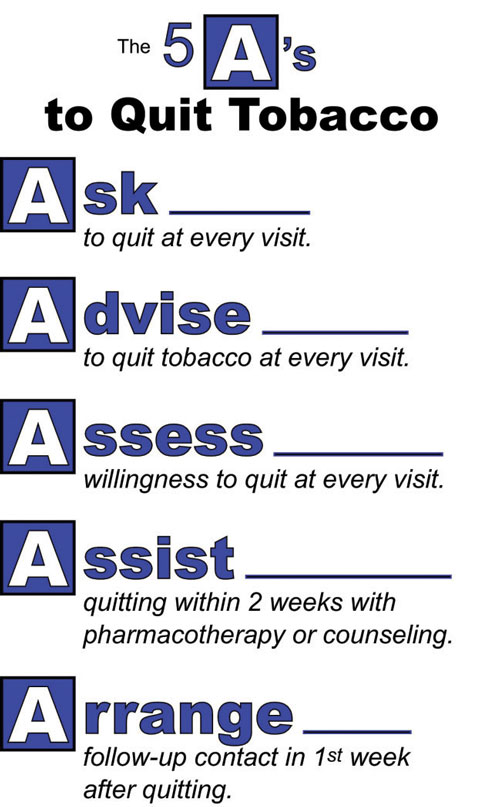 |
| Get the conversation started with these five A’s to quitting tobacco. Image: National Cancer Institute |
Smoking Cessation Strategies
Only 20% of smokers will ask for help with tobacco cessation, and for those who attempt quitting tobacco use without assistance, only 10% will be effective long term.12 Recent research has clarified the addictive nature of nicotine, comparing the dependence to that caused by opiates, cocaine or other illicit drugs.1,2,12 Pharmacologic and counseling strategies are now the cornerstone of tobacco cessation programs and, taken in combination, can achieve the highest rates of smoking cessation.12
Unless there is an obvious contraindication, every adult patient making an attempt at smoking cessation should be offered pharmacologic therapies to improve their chances of success.12 First-line therapies approved by the FDA include six agents: Wellbutrin SR (sustained-release bupropion, GlaxoSmithKline), Chantix (varenicline, Pfizer) and four nicotine replacement therapies (NRTs). These are FDA-approved for adults ages 18 and over who want to quit smoking.13 Three types of NRTs are approved by the FDA for consumers to buy OTC: nicotine gum, transdermal nicotine patch and nicotine lozenge products. There is one prescription-only nicotine replacement product, under the brand name Nicotrol (Pfizer), which is available both as a nasal spray and an oral inhaler.
NRTs should be used for a short time to help the patient manage nicotine cravings and withdrawal.
Interventions to help smoking and tobacco product cessation should be considered a standard of good practice. Tobacco dependence is a chronic condition, but the evidence suggests safe and effective therapeutic options are available to help aid patients in quitting. Excellent resources are available at http://smokefree.gov.
|
1. Centers for Disease Control and Prevention. 2010 Surgeon General’s Report—how tobacco smoke causes disease: the biology and behavioral basis for smoking-attributable disease. Atlanta, GA: 2010. 2. Benowitz NL, Brunetta PG. Smoking hazards and cessation. In: Broaddus VC, Mason RJ, Ernst JD, et al., eds. Murray and Nadel’s Textbook of Respiratory Medicine. 6th ed. Philadelphia: Elsevier Saunders; 2016. 3. O’Connor RJ, McNeill A, Borland R, et al. Smokers’ beliefs about the relative safety of other tobacco products: findings from the ITC collaboration. Nicotine Tob Res. 2007;9(10):1033-42. 4. Lindblad BE, Håkansson N, Wolk A. Smoking cessation and the risk of cataract: a prospective cohort study of cataract extraction among men. JAMA Ophthalmol. 2014;132(3):253-7. 5. Solberg Y, Rosner M, Belkin M. The association between cigarette smoking and ocular diseases. Survey of ophthalmology. 1998;42(6):535-47. 6. Prignot JJ, Sasco AJ, Poulet E, et al. Alternative forms of tobacco use. Int J Tuberc Lung Dis. 2008;12(7):718-27. 7. Rickert WS, Wright WG, Trivedi AH, et al. A comparative study of the mutagenicity of various types of tobacco products. Regul Toxicol Pharmacol. 2007;48(3):320-30. 8. Akl EA, Gaddam S, Gunukula SK, et al. The effects of waterpipe tobacco smoking on health outcomes: a systematic review. Int J Epidemiol. 2010;39(3):834-57. 9. Blachman-Brauna R, Del Mazo-Rodrígueza RL, López-Sámanoa G, Buendía-Roldánb I. Hookah, is it really harmless? Respiratory Medicine. 2014;108(5):661-7. 10. Yamin CK, Bitton A, Bates DW. E-cigarettes: a rapidly growing Internet phenomenon. Ann Intern Med. 2010;153(9):607-9. 11. Wollscheid KA, Kremzner ME. Electronic cigarettes: safety concerns and regulatory issues. Am J Health Syst Pharm. 2009;66(19):1740-2. 12. Black JH. Evidence base and strategies for successful smoking cessation. J Vasc Surg. 2010;51(6):1529-37. 13. US Food and Drug Administration. FDA 101: smoking cessation products. Available at www.fda.gov/ForConsumers/ConsumerUpdates/ucm198176.htm#replacement. Accessed November 22, 2016 |
