Level Up Your TechOptometrists today have more tools than ever at their disposal to help detect, treat and manage disease. To help you keep up with the constant innovation, the September issue of Review of Optometry—our 46th annual technology report—gives readers a rundown on what's new in FAF imaging, visual field testing, ultra-widefield imaging, low vision and more. |
In an era where new technology is quickly evolving, choosing the right visual field techniques and devices is essential for diagnosing and managing optic neuropathies. New algorithms within the Humphrey Visual Field Analyzer deserve a chance in the spotlight. Reducing patient chair time, clinical footprint and technician load while maintaining reliable results is crucial. Many glaucoma providers still prefer using the 24-2 or 10-2 SITA Standard, but there is a benefit to patients and schedules without sacrificing accuracy with the SITA Fast, Faster and 24-2C algorithms. Below, we will look at how the new SITA Faster differs from the SITA Fast. More importantly, is the Humphrey (or Octopus) becoming obsolete? Virtual reality perimetry (VRP) may edge out the Humphrey in a head-to-head comparison, as it offers numerous advantages over our standard automated perimetry (SAP) machines.
For many years, the Humphrey 24-2 has been the mainstay of optometric glaucoma care. Likewise, the 10-2 confirms early glaucomatous defects visualized structurally within the ganglion cell layer (GCL) when using OCT instruments that offer ganglion cell analysis (GCA).
In recent years, the Humphrey 24-2C has been introduced and essentially marries the two tests together in one convenient package. Although the 10-2 continues to be the gold standard for detecting defects corresponding to a loss in the GCL, we often need to choose between the 24-2 and the 10-2 for time and billing purposes. The GCA scans can often show anomalous loss that can be attributed to macular pathologies unrelated to glaucomatous changes. For those with an underlying macular disease, running a 10-2 based on an abnormal GCA can lead to false-positive glaucomatous centralized deficits. In this case, the 24-2C becomes advantageous, as it contains 10 extra data points within the central field that lie just outside areas where macular defects can occur. When performed reliably, the new 24-2C strategy becomes more useful than a standalone 24-2 or 10-2 for early glaucoma and optic neuropathy.
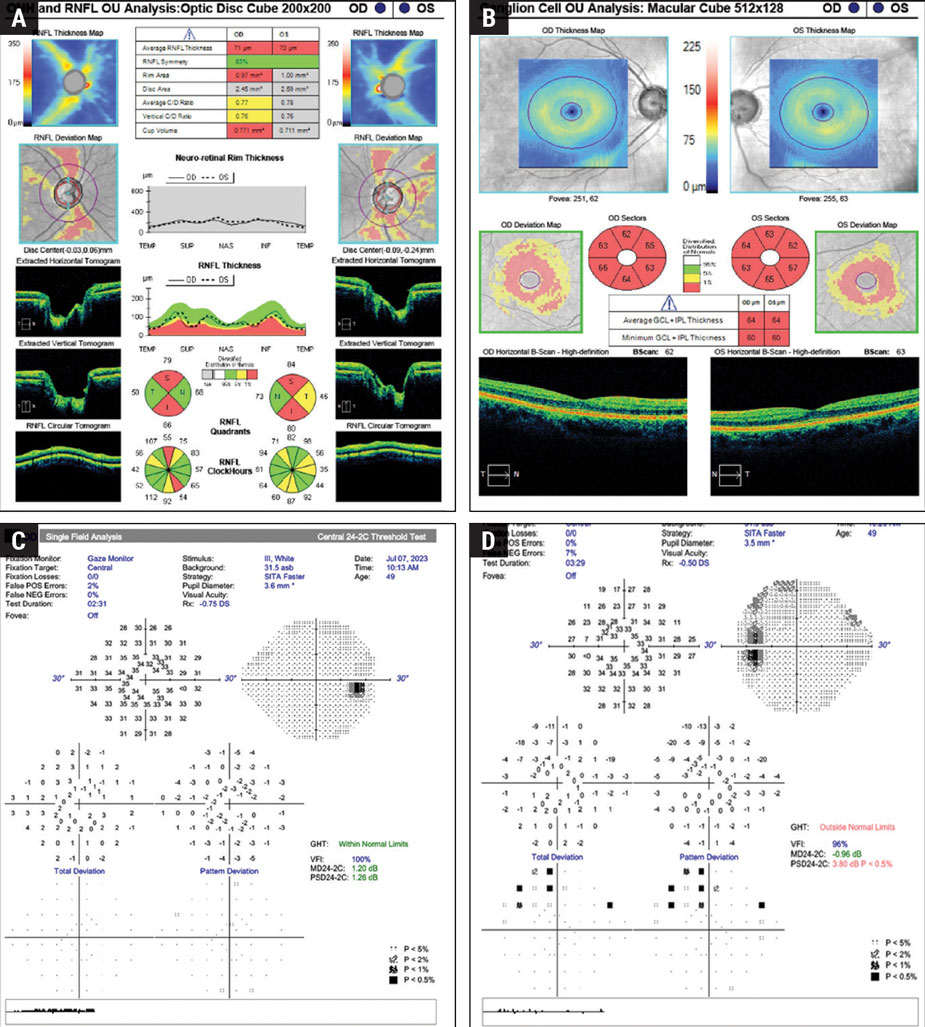 |
Fig. 1. A 49-year-old Caucasian male with no prior diagnosis of glaucoma or family history, IOP 17mm Hg OU with thinner than average pachymetry. (A) OCT RNFL shows an average thickness of 71μm OD and 70μm OS with superior and inferior thinning OU. (B) OCT GCA shows 360° of cell loss OU. (C) Baseline visual field 24-2C SITA Faster OD shows excellent reliability with no glaucomatous depressions. (D) Baseline field 24-2C SITA Faster OS shows excellent reliability and confirms a glaucomatous defect in the superior temporal quadrant forming an early arcuate with no central involvement despite abnormal GCA. Click image to enlarge. |
In a case study looking at the 10-2 vs. the 24-2C in optic neuropathies, there were no perceptible differences between the two—the 24-2C picked up the same defects as the 10-2.1 In this patient, there is considerable loss of the retinal nerve fiber layer (RNFL) with polar thinning and a corresponding loss on the GCA in both eyes at the initial exam (Figure 1). However, when performing a baseline 24-2C SITA Faster, only the left eye was confirmed to have a glaucomatous defect that corresponded with the detected area of loss on ocular computed tomography. In this case, if one of the central data points showed up with a quantifiable depression, the next step could be to order a 10-2 at a follow-up exam, as the functional defects are not correlating to the structural defects in the right eye, despite testing reliability.
To further confirm the extent of central ganglion loss, a 10-2 can be performed but is not necessary, as it would not detect any additional glaucomatous defects that were not visualized on a 24-2C and will not alter the course of treatment.1 A 24-2 SITA Fast would likely correlate with the 24-2C superior temporal defect in OS (Figure 1C and D). However, a 24-2 SITA Fast is not able to test the central area for early glaucomatous defects within the GCL. In those with pre-perimetric or early-stage glaucoma, the 24-2C has shown to be as reliable as the 10-2 for initiating treatment based on a baseline field due to the improved reliability, while reducing the testing time and including central data points.2 This means that we can reliably diagnose and initiate treatment almost three to six months sooner when using a 24-2C than when using a 24-2 as the baseline field.
SITA Fast vs. Faster 24-2
The SITA Standard has been the gold standard for glaucoma visual field testing since its introduction. To reduce patient fatigue, increase reliability and reduce chair time, the SITA Fast was later introduced. Much like how the SITA Standard replaced Full Threshold by reducing the testing time by 50%, the SITA Faster is intended to replace the SITA Fast.3 SITA Fast has also replaced the Fastpac. Eventually, the only option that will be available for the 24-2 test will be the SITA Standard and the new SITA Faster.
To create the SITA Faster, several minor changes were made to the SITA Fast algorithm. Unlike the Full Threshold, SITA Standard and SITA Fast, which use a stimulus of 25dB in the first stimuli of each quadrant, the SITA Faster reduces the brightness to correlate with the patient’s age.4 Because of this, the number of stimuli presented to an older patient is reduced and results in a lower test duration. A patient with mild to moderate optic nerve disease will have an average test time of two minutes, while those with more advanced defects will be longer but less than a SITA Standard. The new algorithm uses the gaze tracker to check the blind spot rather than presenting stimuli. False-negative catch trials were eliminated.
The SITA Faster also saves time by eliminating the time between unseen stimuli, and it no longer retests areas of initial non-response.4 However, these factors should be considered when testing those with conditions that would result in a limited reaction time.
In a study comparing the SITA Faster and SITA Fast with the SITA Standard, the only quantifiable difference observed was a small change in the false-positive rates.3 The SITA Standard has slightly lower false-positive rates than both due to its positive start bias, which involves showing easier stimuli first to help promote a patient’s willingness to engage positively with the test. In contrast, the SITA Fast and Faster are more likely to result in both eyes having equal reliability for interpretation than the Standard. This is in large part due to the observation that patients will usually do well on the first tested eye, only to become less reliable due to testing fatigue on the second eye when using SITA Standard.
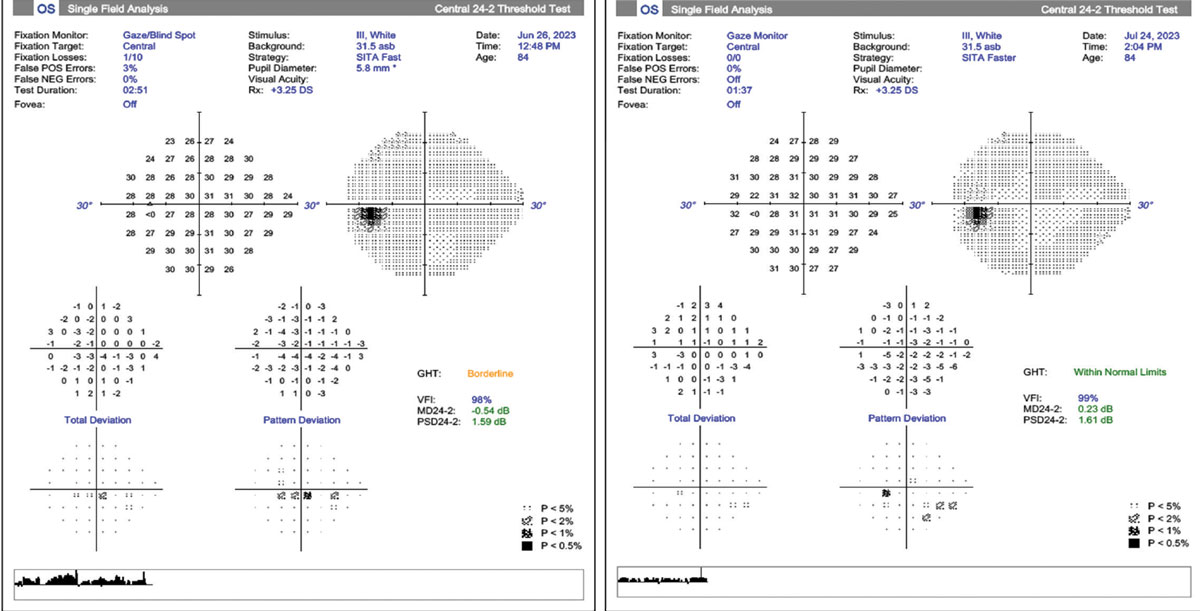
Another study observed that SITA Fast and Standard gave similar results when compared with SITA Faster, finding that the visual field index between all three stayed the same, aiding the reliability, but concluded that the algorithms are not interchangeable for following advanced disease progression between examinations.5 As a result, when comparing previously obtained SITA Fast results with the newer SITA Faster, we see that the testing time reduces by nearly 50% and the reliability of the test further improves with the Faster (Figure 2). However, the defects between the two fields are not comparable or repeatable despite being performed a month apart. The pattern standard deviation values are roughly the same, suggesting high reliability of the test taker.
Based on this example, we can see evidence to support one study’s observation that the SITA Faster tends to show a similar yet smaller-sized field deficits than the SITA Fast, suggesting the two testing modalities are likely not interchangeable for those with advanced glaucoma.4
SITA Faster is a viable option when testing glaucoma suspects up to moderate stages of glaucoma, but the SITA Standard should be used for those with more significant field loss. The Standard allows the patient more response time, which helps detect smaller changes in the field that may signal progression on current therapy. When paired with the 24-2C modality, the SITA Faster is a great option to screen those who have risk factors for glaucoma or are showing pre-perimetric thinning on nerve fiber analysis and/or ganglion cell analysis.
 |
|
Fig. 2. Two examples of 24-2 visual fields of a patient with ocular hypertension Left: SITA Fast field shows good reliability with low fixations losses, low false-positives and a borderline glaucoma hemifield test. There is a small inferior central cluster defect questionable for early glaucoma. Right: One-month follow-up using SITA Faster shows no fixations losses, no false-positives and a glaucoma hemifield test within normal limits. The field does not confirm the previous central defect but reveals a shallow inferior nasal cluster defect. Click image to enlarge. |
Virtual Reality Perimetry vs. the Gold Standard (Humphrey)
The use of VRP in the detection of visual field defects was first introduced in 2018. During the COVID-19 pandemic, VRP gained significant traction in managing glaucoma patients due to its portability, convenience, lower entry price point and space-saving capabilities when compared with SAP.
Studies have shown that frequent field testing is essential in the detection and management of rapidly progressing individuals in the initial stages of glaucoma diagnosis.6 One study recommended performing an average of six visual field tests within the first two years of diagnosis to establish a baseline.7 This follow-up schedule can be a burden to both the patient and clinic if performed using SAP. In these circumstances, VRP becomes an attractive testing modality for the patient and provider.
VRP uses head-mounted devices to administer fields to patients in-office and eventually in the convenience of their home. These devices provide more reliable and repeatable data compared with similarly used tablet-based visual fields for at-home testing, as the lighting and gaze tracking is more accurate.8
Numerous studies have shown VRP produces comparable results with high correlations to SAP testing when diagnosing and managing glaucoma patients.6,8-12 A study evaluating the VisuAll (Olleyes) head-mounted perimetry device in glaucoma patients showed significant correlation in the mean sensitivity when compared to Humphrey Field Analyzer.9 Another study evaluating the Advanced Vision Analyzer (Elisar Vision) head-mounted perimetry device showed similar threshold values to the HVF, suggesting high reliability for detecting defects.10 A different study comparing the Vivid Vision Perimetry with the Humphrey Field Analyzer in those with open angle glaucoma and glaucoma suspects also compared favorably.
Other products on the market include the Smart System VR Headset (M&S Technologies) and VF2000 (Micro Medical Devices). The newest device is the Heru VR, which uses immersive augmented reality. According to a study comparing Heru’s visual field to SITA Standard, the Heru field results were repeatable and comparable with those obtained with SAP Humphrey.13,14
A similarity between all currently available VRP devices is their ability to export results to electronic health records systems using PDFs, making it easy to compare prior results from SAP to VRP. With any visual field test, the reliability of the patient is only part of the equation. Comparing subjective results to objective results is still reliant on the providers interpretation.
Despite the inherent advantages of VR technology, headset devices are not without their disadvantages. Most of the research studies currently available are preliminary in nature, sponsored by the developers of the devices and use small sample sizes.6-8 Moreover, there are multiple VRP devices with different features and algorithms in the current market, making it more challenging to perform large-scale studies comparing these systems with each other, as well as with SAP. Another limitation to VRP is the observance of low sensitivity in screening for early glaucoma, though relatively high sensitivity is noted when screening those with moderate to severe glaucoma.8 In time, large-scale prospective studies with progression analysis will be important to confidently validate the accuracy and reproducibility of VRP systems in comparison with SAP.
There are several benefits that outweigh any disadvantage to VRP that are not as easily recognized from the exterior of these petite technology-packed packages. An appealing aspect includes higher quality user experience compared to SAP, even though certain devices have longer test durations.8-10 VRP allows patients to use more comfortable positioning when performing the test compared with SAP, where patients must maintain a stable head position throughout the duration of the test. Most VRP devices offer accurate gaze tracking using infrared lighting and standard background illumination comparable to that of SAP, which can increase the reliability of the results.6,8
Headset perimetry is an excellent testing method for patients with a history of previously unreliable SAP results, particularly those who have physical limitations that were unable to be tested in the past. VRP can also reduce the clinical burden to practices by reducing technician monitoring time required for each patient when using SAP devices. These devices are also more portable and cost-effective compared to SAP. The average price found for currently available devices started around $10,000, nearly half the cost of SAP. VRP is also ideal for mobile optometric clinicians who care for nonambulatory communities, such as those in nursing homes.
 |
|
|
Takeaways
When looking at current research, the 24-C SITA Faster has proven to be as reliable as the 10-2 for diagnosing early glaucomatous centralized deficits in the ganglion cell layer, but the 10-2 should still be used for monitoring those with advanced glaucoma. The SITA Fast or Faster technique is better for patients who have been unreliable on the SITA Standard, or have had a history of being unable to sit for the duration of the test. VRP shows promise for patients with compromised mobility, clinics with small footprints and mobile optometric physicians. Ultimately, it remains up to the provider to determine their own diagnostic comfort level with new field strategies and decide if a VRP device is beneficial to their mode of practice.
Dr. Banister is an optometrist at The Villages VA Outpatient Clinic in The Villages, FL. She is a graduate of Pennsylvania College of Optometry at Salus University and completed her residency at the Bay Pines VA Healthcare Center in Bay Pines, FL. Dr. Brennan is an optometrist at the Tucson VAMC and an adjunct clinical professor at Ohio State College of Optometry and Marshall B. Ketchum University. He received his undergraduate degree at the University of Utah and optometric degree at Western University College of Optometry. Dr. Brennan completed his residency at the Malcolm Randall VAMC in Gainesville, FL. Dr. Fisher is an optometrist and supervisor at The Villages VA Outpatient Clinic in The Villages, FL. He is a graduate of Midwestern University Arizona College of Optometry and completed his residency in primary care and low vision at the Lake City VA Medical Center in Lake City, FL. Dr. Nguyen is an optometrist at the Phoenix VA Healthcare System. She is a graduate of Midwestern University Arizona College of Optometry and completed her residency at the Malcom Randall VAMC in Gainesville, FL. Dr. Karunathilake is an optometrist at the Lake City VAMC in Lake City, FL, where she serves as the residency coordinator and low vision clinic director. She maintains five adjunct faculty appointments at various colleges of optometry throughout the country. They have no financial disclosures.
1. Haner NU, Dysli C, Muck MR. Imaging in retinal vascular disease: A review. Clin Experiment Ophthalmol. 2023;51:217-28. 2. Patel SN, Shi A, Wibbelsman TD, Klufas MA. Ultra-widefield retinal imaging: an update on recent advances. Ther Adv Ophthalmol. 2020;(12)1-12. 3. Choudhry N, Duker JS, Freund KB, et al. Classification and guidelines for widefield imaging: recommendations from the International Widefield Imaging Study Group. Ophthalmol Retina. 2019;3:10:843-9. 4. Calvo CM., Hartnett ME. The utility of ultra-widefield fluorescein angiography in pediatric retinal diseases. Int J Retin Vitr. 2018;4(21). 5. Midena E., Marchione G, Digiorgio S, et al. Ultra-wide-field fundus photography compared to ophthalmoscopy in diagnosing and classifying major retinal diseases. Sci Rep. 2022;12:19287. 6. Kumar V, Surve A, Kumawat D, et al. Ultra-wide field retinal imaging: a wider clinical perspective. Indian J Ophthalmol. 2021;69:824-35. 7. Salz JJ, Seibel BS. Screening with widefield fundus photography. Widefield technology has value for a practice’s patients, efficiency and bottom line. Ophthamology Management. June 1, 2019. Accessed August 16, 2023. 8. Purbick RM, Izadi S. Gupta A, Chong NV. Comparison of Optomap ultrawide-field imaging versus slit-lamp biomicroscopy for the assessment of diabetic retinopathy. Clin Ophthalmol. 2014;8:1413-7. 9. Wilson PJ, Ellis JD, MacEwen CJ, et al. Screening for diabetic retinopathy: a comparative trial of photograph and scanning laser ophthalmoscopy. Ophthalmologica. 2010;224:251-7. 10. Neubauer AS, Kernt M, Haritoglou C, et al. Nonmydriatic screening laser ophthalmoscopy (optomap). Graefes Arch Clin Exp Ophthalmol. 2008; 246:229-35. 11. Wessel MM, Aaker GD, Parlitis G, et al. Ultra-wide field angiography improves the detection and classification of diabetic retinopathy. Retina. 2012;32(4):785-91 12. Silva PS, Cavallerano JD, Sun JK, et al. Peripheral lesions identified by mydriatic ultrawide field imaging: distribution and potential impact on diabetic retinopathy severity. Ophthalmology. 2013;120(12):2587-95. 13. Silva PS, Cavallerano JD, Tolls D, et al. Potential efficiency benefits of nonmydriatic ultrawide field retinal imaging in an ocular telehealth diabetic retinopathy program. Diabetes Care. 2014;37(1):50-5. 14. Price LD, Au S, Chong NV. Optomap ultrawide field imaging identifies additional retinal abnormalities in patients with diabetic retinopathy. Clin Ophthalmol. 2015;9:527-31. 15. Aiello LP, Odia I, Glassman AR, et al. Comparison of early treatment diabetic retinopathy study standard 7-field imaging with ultrawide-field imaging for determining severity of diabetic retinopathy. JAMA Ophthalmol. 2019;137(1):65-73. 16. Silva PS, Cavallerano JD, Haddad NMN, et al. Peripheral lesions identified on ultrawide field imaging predict increased risk of diabetic retinopathy progression over four years. Ophthalmology. 2015;122:949-56. 17. Hirano T, Imai A, Kasamatsu H, et al. Assessment of diabetic retinopathy using two ultra-wide-field fundus imaging systems, the Clarus and Optos systems. BMC Ophthalmol. 2018;18(1):332. 18. Marcus DM, Silva PS, Liu D, et al. Association of predominantly peripheral lesions on ultra-widefield imaging and the risk of diabetic retinopathy worsening over time. JAMA Ophthalmol. 2022;140(10):946-54. 19. Silva PS, Liu D, Glassman AR, et al. Assessment of fluorescein angiography nonperfusion in eyes with diabetic retinopathy using ultrawide field retinal imaging. Retina. 2022;42:1302-10. 20. Yusuf IH, Lotery AJ. Thinking outside the circle-the potential value of ultra-widefield imaging. JAMA Ophthalmol 2022;140(10):955-6. 21. Nicholson L, Ramu J, Chan EW, et al. Retinal nonperfusion characteristics on ultra-wide field angiography in eyes with severe nonproliferative diabetic retinopathy and proliferative diabetic retinopathy. JAMA Ophthalmol. 2019;137:626-31. 22. Lasave AF, Shoughy SS, Kozak I, Arefalo, JF. When ultra-widefield retinal imaging is most useful. Retina Today. 2019;36-40. 23. Wykoff CC, Nittala MG, Zhou B et al. Intravitreal afilbercept for retinal nonperfusion in proliferative diabetic retinopathy: outcomes from the randomized recovery trial Ophthalmol Retina. 2019;3:1076-86. 24. Campochiaro PA. Low risk to retina from sustained suppression of VEGF. J Clin Invest. 2019;129(8):3029-31. 25. Pichi F, Carreño E, Pavesio C, et al. Consensus-based recommendations for OCT angiography reporting in uveitis. Br J Ophthalmol. 2023;107(7):959-65. 26. Munk MR, Kashani AH, Tadayoni R, et al. Recommendation for OCT angiography reporting in retinal vascular disease. A Delphi approach by international experts. Opthalmol Retina. 2022;6(9):753-61. 27. Li M, Mao M, Wei D, et al. Different scan areas affect the detection rates of diabetic retinopathy lesions by high-speed ultra-widefield swept-source optical coherence tomography angiography. Front Endocrinol (Lausanne). 2023;14:1111360. 28. Singer M, Tan CS, Bell D, Sadda SR. Area of peripheral retinal nonperfusion and treatment response in branch and central retinal vein occlusion. Retina. 2014;34(9):1736-42. 29. Campochiaro PA, Bhistkul RB, Shapiro H, Rubio RG. Vascular endothelial growth factor promotes progressive retinal nonperfusion in patients with retinal vein occlusion. Ophthalmology. 2013;120(4):795-802. 30. Tan TE, Ibrahim F, Chandrasekaran PR, Teo KYC. Clinical utility of ultra-widefield fluorescein angiography and OCT angiography for retinal vein occlusions. Front Med (Lausanne). 2023;10:1110166. 31. Sivaprasad S, Amoaku WM, Hykin P. The Royal College of Ophthalmologist Guidelines on retinal vein occlusions: executive summary. Eye (Lond). 2015;29(12):1633-8. 32. Nicholson L, Vazquez AC, Patrao NV, et al. Retinal nonperfusion in the posterior pole is associated with increased risk of neovascularization in central retinal vein occlusion. Am J Ophthalmol. 2017;182:118-25. 33. Nicholson L, Vazquez-Alfageme C, Sen P, et al. The clinical relevance of ultra-widefield angiography findings in patients with central retinal vein occlusion and macular oedema receiving anti-VEGF therapy. Eye (Lond). 2022;36(5):1086-93. 34. Witmer MT, Cho M, Favarone G, et al. Ultra-wide field autofluorescence imaging in non-traumatic rhegmatogenous retinal detachment. Eye (Lond). 2012;26(9):1209-16. 35. Choudhry N, Golding J, Manry MW, Rao RC. Ultra-widefield steering-based spectral-domain optical coherence tomography imaging of the retinal periphery. Ophthalmology. 2016;123:1368-74. 36. Alone A, Chandra K, Chhablani J. Wide-field imaging-an update. Indian J Ophthalmol. 2021;69(4):788-9. 37. Temkar S, Azad SV, Chawla R, et al. Ultra-widefield fundus fluorescein angiography in pediatric retinal vascular diseases. Indian J Ophthalmol. 2019;67(6):788-94. 38. Lee SJ, Yang KM, Lee KB, Park NC. Design of illumination system using characterized illuminances for smartphone-based fundus camera. Opt Lasers Eng. 2023;168:107664. 39. Iqbal, U. Smartphone fundus photography: a narrative review. Int J Retin Vitr. 2021;7(44). 40. Sedova A, Hajdu D, Datlinger G, et al. Comparison of early diabetic retinopathy staging in asymptomatic patients between autonomous AI-based screening and human-graded ultra-widefield color fundus images. Eye. 2022;36:510-6. |
