 History
History
A 27-year-old black female presented following an ER visit for a chief complaint of a painful left eye, which had persisted for one hour. The patient explained that this had happened twice before—both times upon waking in the morning.
Further, she informed us that these episodes seemed to begin following a fingernail injury to her left eye three months earlier. She had no contributory systemic history, and no known allergies.
Diagnostic Data
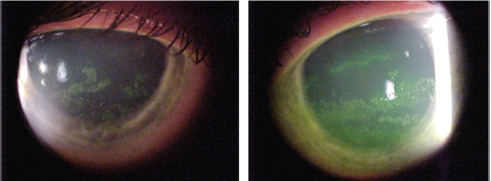
Slit-lamp images of our 27-year-old patient (OD left, OS right) who presented emergently with a
painful left eye. What is your diagnosis?
Her best-corrected visual acuity was 20/20 OD and 20/40 OS at distance and near. External examination findings were normal, with no evidence of afferent pupillary defect in either eye.
Her intraocular pressure measured 14mm Hg OU. The dilated fundus examination was normal. The pertinent biomicroscopic examination findings are illustrated in the photographs.
Your Diagnosis
How would you approach this case? Does the patient require any additional testing? What is your diagnosis?
How would you manage or treat this patient? What is the likely prognosis?
Thanks to Marc D. Myers, OD, of Coatesville, Pa., for contributing to this case.
Discussion
Additional testing might include rose bengal staining to assess for devitalized cells, and corneal sensitivity testing to ensure adequate sensation.
The diagnosis in this case is recurrent corneal erosion (RCE) OS secondary to the abrasion caused by a finger poke three months earlier.
RCE is characterized by one or more episodes of spontaneous corneal epithelial breakdown.1-4 The symptoms typically occur upon waking, with episodes that vary in both severity and duration.3,4 RCE can be classified as either primary or secondary, depending whether the epithelial basement membrane defect is intrinsic or acquired.3,4
Following most superficial insults, the corneal epithelium has the ability to heal within 24 to 48 hours.1,5 If the whirling Bowman’s membrane or the lattice-like structure of the stroma is not involved, no scarring typically ensues.5
After a wound occurs, damaged epithelial cells lose their microvilli, basal cells flatten, and wing and superficial cells shed their tight junctions––liberating their glycogen stores. Within an hour, neutrophils are evident in the tear film and anterior wound area.4,5 Fifteen hours into the process, epithelial cells can be seen sliding into the damaged area. The increasing number of neutrophils is thought to remove cellular debris and facilitate rapid healing.
The majority of the defect often re-epithelializes within 24 hours, and almost all of the neutrophils migrate out of the tissue.4,5 Within six to 14 days, the epithelium regains its normal thickness; but attachment to Bowman’s layer by hemidesmosomes takes approximately six weeks.4
Patients with a history of chronic corneal abrasions are more prone to RCE due to poor hemidesmosome formation.1,2 When these hemidesmosomal anchoring fibers are not properly established, the epithelium can spontaneously “peel off.” This happens most frequently upon awakening, as the patient first opens his or her eyes.1,2,6 Patients who have no history of a corneal abrasion, but suffer from corneal dystrophies (e.g., Cogan’s microcystic, map-dot-fingerprint, Meesmann corneal, Reis-Bucklers, honeycomb, granular or lattice), also are susceptible to RCE.1,2,6-9
There are several approaches for treating RCE: pressure patching; bandage soft contact lenses; bland, hyperosmotic/hypertonic and antibiotic ointments and drops; topical non-steroidal and steroidal anti-inflammatory preparations; and cycloplegic drops for discomfort, when necessary.3,8-23 Topical autologous serum is a newer therapy that repairs the injured epithelium.24,25
When topical medical therapy fails, oral antibiotic medications (i.e., doxycycline) may be helpful.12,13 Non-invasive management of recalcitrant cases may include care of the associated lid pathology. Surgical procedures, such as debridement of loose epithelium, alcohol debridement of the corneal epithelial basement membrane, anterior stromal puncture, botulinum toxin injections, diamond burr superficial keratectomy, superficial laser therapeutic keratectomy (PTK), penetrating keratoplasty (PK) and lamellar surgery, can be employed in cases that fail to respond to traditional modalities.19-33
As with any open wound, there always is the risk of invasion by infectious organisms, which is why topical antibiotics are the mainstay of treatment for any epithelial corneal defect.9,10 There is no reason to withhold prophylactic treatment with the fourth-generation fluoroquinolones; the solutions are effective on a dosing regimen of one drop QID. Also, apply ointments generously BID––both for additional contact time and to add a lubricating effect. One recent evaluation has determined that these agents have no impact on preventing corneal re-epithelialization.10
We medicated the patient with topical antibiotics and copious lubricants. Additionally, we considered the application of a bandage contact lens or corneal collagen crosslinking. However, neither intervention was necessary because healing ensued shortly after the start of primary treatment.
1. Remington LA. The Cornea and Sclera. In: Clinical Anatomy of the Visual System. Newton, Mass.: Butterworth-Heinemann; 1998;9-29.
2. Fujikawa LS, Nussenblatt RB. Recurrent and Chronic Corneal Epithelial Defects. In: Abbott RL. Surgical Intervention in Corneal and External Diseases. New York: Grune and Stratton Inc.; 1987:59-67.
3. Kirkwood BJ. Recurrent corneal erosion: characteristics and management options. Insight. 2007 Oct-Dec;32(4):14-7.
4. Das S, Seitz B. Recurrent corneal erosion syndrome. Surv Ophthalmol. 2008 Jan-Feb;53(1):3-15.
5. Binder, PS, Wickham GM, Zavala EY, et al. Corneal Anatomy and Wound Healing. In: Barraquer, JI, Binder PS, Buxton JN (eds.). Symposium on Medical and Surgical Diseases of the Cornea. St. Louis: CV Mosby Company; 1980:1-35.
6. François J. Recurrent dystrophic erosion of the corneal epithelium. Ophthalmologica. 1978; 177(3):121-33.
7. Rosenberg ME, Tervo TM, Petroll WM, et al. In vivo confocal microscopy of patients with corneal recurrent erosion syndrome or epithelial basement membrane dystrophy. Ophthalmology. 2000 Mar;107(3):565-73.
8. Kaiser PK. The Corneal Abrasion Patching Study Group. A comparison of pressure patching versus no patching for corneal abrasions due to trauma or foreign body removal. Ophthalmology. 1995 Dec;102(12):1936-42.
9. Ta CN, Chan I, Dhatt HS, et al. Prospective comparison of topical moxifloxacin in eliminating conjunctival bacterial flora following a one-day or one-hour application. J Ocul Pharmacol Ther. 2008 Aug;24(4):427-31.
10. Moshirfar M, Chew J, Werner L, et al. Comparison of the effects of fourth-generation fluoroquinolones on corneal re-epithelialization in rabbit eyes. Graefes Arch Clin Exp Ophthalmol. 2008 Oct;246(10):1455-61.
11. Hirst LW. Pressure patching for corneal abrasions. Ophthalmology. 1997 Feb;104(2):169.
12. Wang L, Tsang H, Coroneo M. Treatment of recurrent corneal erosion syndrome using the combination of oral doxycycline and topical corticosteroid. Clin Experiment Ophthalmol. 2008 Jan-Feb;36(1):8-12.
13. Smith VA, Khan-Lim D, Anderson L, et al. Does orally administered doxycycline reach the tear film? Br J Ophthalmol. 2008 Jun;92(6):856-9.
14. Arbour JD, Brunette I, Boisjoly HM, et al. Should we patch corneal erosions? Arch Ophthalmol. 1997 Mar;115(3):313-7.
15. Webster RG. Corneal Injuries. In: Smolin G, Thoft RA. The Cornea. Boston: Little Brown and Company; 1987:517-27.
16. Patterson J, Fetzer D, Krall J, et al. Eye patch treatment for the pain of corneal abrasion. South Med J. 1996 Feb;89(2):227-9.
17. Liu C, Buckley R. The role of the therapeutic contact lens in the management of recurrent corneal erosions: a review of treatment strategies. CLAO J. 1996 Jan;22(1):79-82.
18. Kanpolat A, Uçakhan OO. Therapeutic use of Focus Night & Day contact lenses. Cornea. 2003 Nov;22(8):726-34.
19. Kaiser PK, Pineda RA. Study of topical nonsteroidal anti-inflammatory drops and no pressure patching in the treatment of corneal abrasions. Ophthalmol 1997 Aug;104(8):1353-9.
20. Watson SL, Barker NH. Interventions for recurrent corneal erosions. Cochrane Database Syst Rev. 2007 Oct 17;(4):CD001861.
21. Rapuano CJ. PTK effective therapy for select group of patients. Ophthalmol Times. 1998;10(8):2-3.
22. Maini R, Loughnan MS. Phototherapeutic keratectomy re-treatment for recurrent corneal erosion syndrome. Br J Ophthalmol. 2002 Mar;86(3):270-2.
23. Van Westenbrugge JA. Small spot phototherapeutic keratectomy for recurrent corneal erosion. J Refract Surg. 2007 Sep;23(7):721-4.
24. Holzer MP, Auffarth GU, Specht H, Kruse FE. Combination of transepithelial phototherapeutic keratectomy and autologous serum eyedrops for treatment of recurrent corneal erosions. J Cataract Refract Surg. 2005 Aug;31(8):1603-6.
25. Del Castillo JM, de la Casa JM, Sardina RC, et al. Treatment of recurrent corneal erosions using autologous serum. Cornea. 2002 Nov;21(8):781-3.
26. Reidy JJ, Paulus MP, Gona S. Recurrent erosions of the cornea: epidemiology and treatment. Cornea. 2000 Nov;19(6):767-71.
27. Eschstruth P, Sekundo W. Recurrent corneal erosion: different treatment options with the excimer laser with emphasis on aggressive PTK. Ophthalmologe. 2006 Jul;103(7):570-5.
28. Lyon F, Ellingham RB. Alcohol debridement for recurrent corneal erosions. Eye. 2007 Mar;21(3):439-40.
29. Shah S, Browning AC, Dua HS. Alcohol delamination of the corneal epithelial basement membrane in the human eye for photorefractive keratectomy (ARVO abstract). Invest Ophthalmol Vis Sci. 2003 Feb;44(2):510-3.
30. Browning AC, Shah S, Dua HS. Alcohol debridement of the corneal epithelium in PRK and LASEK: an electron microscopic study. Inves Ophthalmol Vis Sci. 2003 Feb;44(2):510-3.
31. Dua HS, Lagnado R, Raj D, et al. Alcohol delamination of the corneal epithelium: an alternative in the management of recurrent corneal erosions. Ophthalmology. 2006 Mar;113(3):404-11.
32. Heyworth P, Morlet N, Rayner S, et al. Natural history of recurrent erosion syndrome, 4 year review of 117 patients. Br J Ophthalmol. 1998 Jan;82(1):26-8.
33. Mackie IA. Successful management of three consecutive cases of recurrent corneal erosion with botulinum toxin injections. Eye. 2004 Jul;18(7):734-7.
