Proper contact lens care and patient compliancewith lens care instructions, recommended lens replacement schedules and follow-up carehas always been considered important in optometric practice. Nevertheless, as many as 32% to 80% of patients do not totally comply with their doctors instructions.1-15
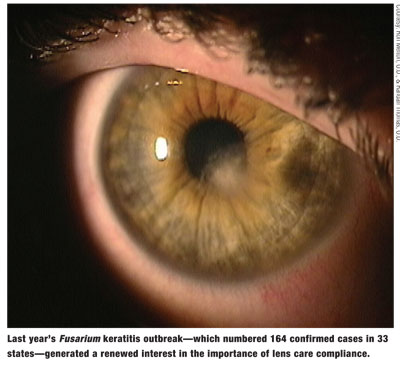
However, last years Fusarium keratitis outbreakwhich resulted in 164 confirmed cases by the Centers for Disease Control and Prevention (CDC) in 33 states and one United States territorygenerated a renewed interest in the importance of compliance to lens care.16 Bausch & Lombs withdrawal of ReNu MoistureLoc formula from the marketused exclusively in 57% of these cases (with possible use in many other cases)has obviously impacted the incidence of this condition.
This outbreak focused attention on the fundamental issue of convenience vs. compliance with the prescribed care regimen and care instructions. Consumers are increasingly interested in the convenience and price of private label solutions. In a recent study by Jobson Research, the fact that contact lenses were considered a hassle was the second most common reason (next to discomfort) for discontinuation of lens wear by the 1,232 respondents to this survey.17
Indeed, factors implicated in the outbreak of Fusarium keratitisin addition to a possible interaction between the MoistureLoc formula and the contact lenses and lens caseincluded the omission of important steps in the care process:18
1. Not using fresh solution every day.
2. Not rubbing the lenses after removal.
3. Not adhering to recommended replacement schedule and overwearing lenses.
(Take note that ReNu MultiPlus retained a high level of biocidal activity under the same conditions.)
Therefore, were left with one obvious question: Has this outbreak changed how practitioners and their employees educate their patients about contact lens care?
The Big Question
I posed this question to the 55-member Advisory Committee of the GP Lens Institute (GPLI). The GPLI is the educational division of the Contact Lens Manufacturers Association. This group of practitioners was selected to participate due to their reputation as experts in the contact lens industry with expertise in all types of contact lens materials (soft and GP) and designs.
Specifically, they answered the following question: Have you made any changes in how you educate contact lens patients since the Fusarium keratitis outbreak (i.e., educational materials, case replacement, importance of compliance, etc.)? Why or why not?
Of the 55 members, 27 members (49.1%) responded to this one-question e-mail surveytheir names are listed at the end of this article. Of these respondents, 15 (55.5%) indicated that they had changed how they educate their patients. The remaining 12 (44.4%) indicated that they made no change in how they approached patients.
A common response from those practitioners who changed how they approached patients: They did not necessarily change the information they presented; rather, they changed the emphasis of what they presented. Specifically, they emphasize these seven points:
1. Use Compatible Solutions
Non-compliance with lens care has been identified as a risk factor for corneal staining.19 An incompatible solution could lead to problems of corneal disruption. Some solutions, such as Opti-Free RepleniSH multipurpose solution (Alcon) and Aquify multipurpose solution (CIBA Vision), specifically mention silicone-hydrogel lens materials as an indication for these products.
Make sure patients understand what complications are possible with non-compliance with lens care; show them photographs of redness, infection, inflammation and staining to emphasize the point. Obviously, tap water is contraindicated with soft lenses. Likewise, with the risk of Acanthamoeba keratitis, tap water should not be used with GP lensesespecially after disinfection. To provide patients with even more information on complications, direct them to the lens manufacturers Web site. (See Patient Education Sites on the Web.")
If the patient is a child, teen or even a young adult and has parents or siblings who are contact lens wearers, find out what care system(s) the family uses and determine whether the system(s) is compatible with this patients lenses. If it is not compatible, emphasize to the patient the possible consequences of using this system.
Likewise, be sure that the lens care system you prescribe is readily available; if not, the patient will likely use another product that may or may not be compatible. You can minimize this problem by initially providing patients with a two- to three-month supply of solutions. Also, by selling solutions in your office, you can help ensure that patients continue to use the solutions you prescribed.
If a patient simply tops off the disinfecting solution and does not refill the case with all fresh solution, the risk of eye infection increases. Advise patients to disinfect their lenses at every removal and discard the solutions prior to the expiration date on the bottle.
Patients must also adhere to the recommended maximum storage times with their prescribed disinfection solutions. This usually ranges from seven to 30 days.
3. Replace the Case
The moist environment of a contact lens storage case is veritable greenhouse for microbial growth. Patrick Caroline and Mark Andre found that 42% of patients had culture-positive bacteria growing onto the inner walls of their contact lens cases.20
The presence of biofilma glycocalyx slime secreted by bacteriacan protect microorganisms and make the disinfecting solution less effective.21 As noted, lens cases were also implicated as a possible contributor to the Fusarium outbreak.
Several survey respondents said they now place greater emphasis on regular case replacement, recommending anywhere from quarterly to monthly replacement.
Specifically, they recommend that O.D.s:
Provide several cases at the dispensing visit and additional cases at follow-up and annual examinations.
Instruct patients to replace their cases at every major holiday (i.e., New Years Day, Valentines Day, Easter, Fourth of July, Labor Day and Thanksgiving).
Suggest that patients enroll in Bausch & Lombs Wear & Care Healthy Contact Lens Care Program (http://009f0a5.netsolhost.com or www.bausch.com), in which consumers receive 12 free contact lens cases and an educational DVD.
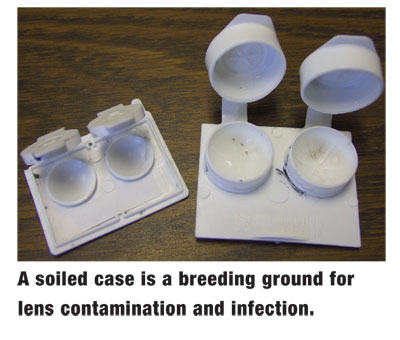
They also emphasize proper care of the contact lens case. This can include showing the patient photographs (or video slit lamp images) of a soiled case (and lenses).
Instruct patients to rinse the case at night and clean it weekly. Weekly cleaning involves rinsing out the case with boiling hot water (and letting it air dry without replacing the tops), or using a surfactant cleaner and digitally scrubbing the case prior to rinsing and air drying.
New lens cases that have anti-microbial properties are being developed. Messrs. Caroline and Andre first reported the use of platinum, silver and carbon molecules impregnated within the matrix of the lens case; silver ions in particular have anti-microbial properties.20 This is the principle behind the Pro-Guard lens case, which accompanies every purchase of AQuify solution. This case has been found to decrease contamination by 40% when used with this specific solution.25 Marietta Vision Specialty Contact Lenses also distributes a contact lens case that has incorporated nanosilver, which helps inhibit multiplication and growth of bacteria and fungi.

4. Emphasize Rub and Rinse
Most of the comments by those surveyed emphasized the importance of digital rubbing upon removal of the lens to remove contaminants. The mechanical effect of digital rubbing, accompanied by rinsing, has been found to dislodge Acanthamoeba from the lens surface.26,27
Miraflow Extra-Strength Daily Cleaner (CIBA Vision), with isopropyl alcohol as an active ingredient, has returned to the market. This is not only an effective cleaner, it also kills both the trophozoite and cyst forms of Acanthamoeba.28
If you allow patients to adhere to the no-rub labeling of certain multipurpose disinfecting solutions, be sure they understand that the lens needs to be rinsed upon removal, not simply placed into the solution. This is a common omission in the patient care process.29
5. Provide Comprehensive Education
Patients must be well informed, starting with the very first visit. This includes verbal presentation of handling, proper cleaning and disinfection, wearing schedule, and normal and abnormal symptoms (and what to do if the latter occurs). Patients who receive a complete demonstration of their recommended care system are less likely to change solution brands.30
Of particular importance: Have the patient repeat your care instructions to ensure they understand them.
Be aware that patients often dont read the written materials you give them, and the small print of the care instructions provided with their care system is a deterrent to reading this information. To that end, have them sign an agreement for compliance (see Lens Care Compliance Agreement.") Such an agreement serves two goals: It helps you educate the patient and it requires them to partner with you to properly care for their lenses.
6. Re-Educate at Follow-Up Visits
Obviously, the educational process only begins at the dispensing visit. Re-educating the patient at every follow-up visit is vital to successful patient compliance. When care procedures are reinforced at all follow-up visits, contamination of contact lenses, care products and cases is reduced from 50% to 6%.31
Follow-up visits are an opportunity to ensure that patients:
Have mastered lens handling.
Are aware of and comply with every step of the care process.
Comply with the recommended wear and replacement schedule.
Still use the care system you recommended.
Receive additional solutions and cases.
Have their questions answered.
Also, consider performing corneal staining at all follow-up visits to help ensure compliance with lens care.
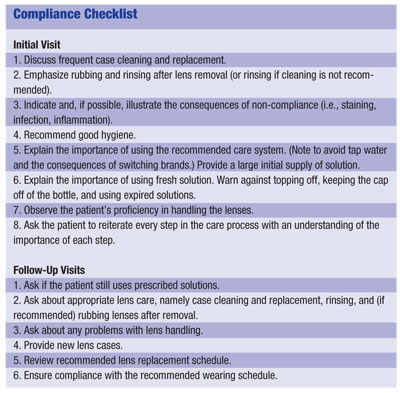
To be sure that you and your employees provide the patient with at least the minimum recommended instructions, use a checklist at the visit and all follow-up visits. (See Compliance Checklist.")
7. Remember Other Important Factors
Emphasize good hygiene. This seems so obvious that we may neglect to underscore the importance of this to patients. The cleanliness of the environment in which the patient handles the lenses and the cleanliness of the work environment are both important. Likewise, hand washing before touching the lenses is an essential step.
Four survey respondents said they switched many of their patients to hydrogen peroxide following the Fusarium outbreak. Since the patient must replace the disk monthly, the doctor can trace patient purchases and verify compliance.
But, more can be done. To optimize compliance, the solution manufacturers could assist patients by making the following changes:
Include a case with each solution purchase.
Increase the font size for the care instructions that accompany the care solution.
Make the expiration dates on solution bottles more visible. On many bottles, the expiration date is almost unreadable.
The Fusarium issue and recent product recalls have changed the way we practice and, most importantly, the way patients have responded to the renewed interest in compliance. The one positive outcome from such a serious outbreak: Many doctors have sharpened the compliance information that they present to their patients.
Since this outbreak, patients generally are more attentive to discussions about proper care, especially the possible ramifications of noncompliance. Many are aware of the Fusarium keratitis issue. Dont disregard this; use it as a motivating force for them to adhere to your recommended care instructions.
In the long run, this outbreak could represent a very constructive outcome for the contact lens industry.
Dr. Bennett is director of student services at the University of MissouriSt. Louis College of Optometry and executive director of the GP Lens Institute.
He thanks the following individuals for their contributions: Art Epstein, O.D.; Bill Edmondson, O.D.; Robert Davis, O.D.; Craig Norman, FCLSA; Roger Tabb, O.D.; Zoraida Fiol-Silva, M.D.; Cary Herzberg, O.D.; Michael Ward, FCLSA; Frank Weinstock, M.D.; Mark Andre, FCLSA; Marlane Brown, O.D.; Doug Blackman, O.D.; Jim Hartzell, O.D.; Sue Resnick, O.D.; Walter Choate, O.D.; Doug Benoit, O.D.; Eric Knutson, O.D.; Barry Eiden, O.D.; Eric White, O.D.; Loretta Szczotka-Flynn, O.D.; Tim McMahon, O.D.; Joe Barr, O.D., M.S.; Lee Rigel, O.D.; Bob Grohe, O.D.; Milton Hom, O.D., Jon Kendall, O.D., Shelley Cutler, O.D.
1. Weisbarth RE,
2. Roth HW. The etiology of ocular irritation in soft lens wearers: distribution in a large clinical sample. Contact Intraoc Lens Med J 1978;4:38-46.
3. Key JE, Mobley CL. Preventing problems with the current care systems. Ophthlmol Clin 1989;2:339-350.
4. Stehr-Green JK, Bailey TM, Brandt FH, et al. Acanthamoeba keratitis in soft contact lens wearers. A case-control study. JAMA 1987 Jul 3;258(1):57-60.
5. Bowden FW, Cohen EJ, Arensten JJ, et al. Patterns of lens care practices and lens product contamination in contact lens associated microbial keratitis. CLAO J 1989 Jan-Mar;15(1): 49-54.
6. Velasco J, Bermudez J. Comparative study of the microbial flora on contact lenses, in lens cases, and in maintenance liquids. Int Contact Lens Clin 1996;23:149-151.
7. Collins MJ, Carney LG. Patient compliance and its influence on contact lens wearing problems. Am J Optom Physiol Opt 1986 Dec;63(12):952-6.
8. Chun MW, Weissman BA. Compliance in contact lens wear. Am J Optom Physiol Opt 1987 Apr;64(4):274-6.
9. Collins MJ, Carney LG. Compliance with care and maintenance procedures amongst contact lens wearers. Clin Exp Optom 1986;69:174-177.
10. Koetting RA, Castellano CF, Wartman R. Patient compliance with EW instructions. Contact Lens Spectrum 1986 Jan;1:23-30.
11. Phillips LJ, Prevade SL. Replacement and care compliance in a planned replacement contact lens program. J Am Optom Assoc 1993 Mar;64(3):201-5.
12. Radford CF, Lehmann OJ, Dart JK. Acanthamoeba keratitis: multicentre survey in
13. Coopersmith L, Weinstock FJ. Current recommendations and practice regarding soft lens replacement and disinfection. CLAO J 1997 Jul;23(3):172-6.
14. Optimize your contact lens options. Contact Lens Spectrum 1995;10:27.
15. Gower L, Stein J, Turner D. Compliance: a comparison of three lens care systems. Optom Vis Sci 1994 Oct;71(10): 629-34.
16. Chang DC, Grant GB, ODonnell K, et al. Fusarium Keratitis Investigation Team. Multistate outbreak of Fusarium keratitis associated with use of a contact lens solution. JAMA 2006 Aug 23;296(8):953-63.
17. 2006 Contact Lens Insight Survey. Jobson Research, 2006.
18. Levy B, Heiler D, Norton S. Report on testing from an investigation of Fusarium keratitis in contact lens wearers. Eye & Contact Lens 2006 Dec;32(6):256-61.
19. Nichols KK, Mitchell GL, Simon KM, et al. Corneal staining in hydrogel lens wearers. Optom Vis Sci 2002 Jan;79(1): 20-30.
20. Caroline PJ, Andre MP. Searching for an antimicrobial contact lens case. Contact Lens Spectrum 2005 Jan;20(1): 56.
21. McLaughlin-Borlace L, Stapleton F, Matheson M, et al. Bacterial biofilm on contact lenses and lens storage cases in wearers with microbial keratitis. J Appl Microbiol 1998 May; 84(5):827-38.
22. Ward MA. Keeping clean cases. Contact Lens Spectrum 2004 Jan;19(1):27.
23. Smythe JL. The forgotten lens care step. Contact Lens Spectrum 2003 Sep;18(9):21.
24. Caroline PJ, Andre MP. Combating the dreaded contact lens case. Contact lens case reports. Contact Lens Spectrum 2000 Apr;15(4):57.
25. Amos C. Clinical testing of the MicroBlock antimicrobial lens case. Optician 2005 Jul 1; 230 (6008): 16-20.
26. Connor CG, Presley L, Fincham SM, et al. The effectiveness of several current soft contact lens care systems against Aspergillus. CLAO J 1998 Apr;24(2):82-4.
27. Liedel KK, Begley CG. The effectiveness of soft contact lens disinfection systems against Acanthamoeba on the lens surface. J Am Optom Assoc 1996 Mar;67(3):135-42.
28. Penley CA, Willis SW, Allen AW. Effects of cleaning and rinsing on the removal of Acanthamoeba from hydrogel lenses. Poster presented at the annual meeting of the
29. Johnson C, Kohler N, Bean B, et al. Rub vs. no rub: what are the costs? Contact Lens Spectrum 2002 July;17(7):24-20.
30. Mummert R. Trends in lens care. Contact Lens Spectrum 1998;13(Suppl):4s-8s.
31. Wilson L, Sawant AO, Simmons RB, Ahearn DG. Microbial contamination of contact lens storage cases and solutions. Am J Ophthalmol 1990 Aug 15;110(2):193-8.
