Optometric SurgeryThe scope of practice has expanded for optometrists in several states over the last few years to include minor ocular surgery and use of lasers. Today, 10 states allow ODs to perform these advanced procedures, which are on their way to becoming ingrained into the profession's DNA. Whether your state already has or has yet to expand its optometric practice scope, this month's issue of Review of Optometry intends to prepare ODs across the country to tackle these new opportunities when their time comes. Check out the other articles featured in the December issue:
|
As scope of practice expansion efforts continue nationwide and more states are passing legislation, a growing number of optometrists are able—many for the first time—to practice to the full extent of their training and abilities, improving the level of care they can offer their patients. Two ocular procedures increasingly being recognized as part of optometry’s scope of practice include laser and minor surgery.
Integrating new procedures into clinical practice can be a challenge requiring time, patience and, in most cases, financial resources. Here, we’ll discuss how ODs can set themselves and their practices up for success.
Scope War Continues
Before we dive into the advice for ODs, let’s review the outcome of several states’ recent battles for expanded practice authority.
Since 2017, six states have passed crucial legislation allowing their optometrists to perform advanced procedures, including laser surgery. From least to most recent, they are Alaska, Arkansas, Wyoming, Mississippi, Virginia and Colorado.
“We have certainly seen the benefit to patients over the years as we’ve seen the practice of optometry grow and change,” says Dana Day, OD, of The Eye Institute of Wyoming and past president of the Wyoming Optometric Association. “It’s hard for me to imagine a time when optometrists didn’t even have the authority to dilate an eye, let alone prescribe any type of therapeutic drops for treatment of infections, inflammation or pressure control. Where would our patients be at this point had scope expansion never occurred? It’s for the benefit of delivering better, more timely eye care to our patients that expansion of scope happens,” he says.
The scope of practice for optometrists employed with the US Department of Veterans Affairs (VA) also expanded this past October when the VA revised guidelines that formerly stated that only ophthalmologists could perform invasive procedures (read the story from our News Feed here). Now, the document states that ophthalmologists or optometrists can perform various types of eye surgery, administer injections and remove lesions, provided it’s allowed by law in the doctor’s state of licensure.
However, just as we have witnessed legislative wins, there have also been temporary setbacks over the years, such as the recent veto of California’s scope expansion bill, AB 2236. The legislation would have granted ODs the authority to perform several advanced procedures including three types of laser surgery—selective laser trabeculoplasty (SLT), capsulotomy and peripheral iridotomy—lesion removal, multiple types of injections and corneal crosslinking (CXL).
When defending his decision to veto the bill, Gov. Gavin Newsom cited concerns regarding education and training, noting that AB 2236 would have allowed ODs to perform the same procedures with one year of training as ophthalmologists perform after three years of training. Optometrists have since disputed this reasoning, arguing that the profession does have the necessary knowledge and skills to safely perform the procedures specified in this legislation.
 |
|
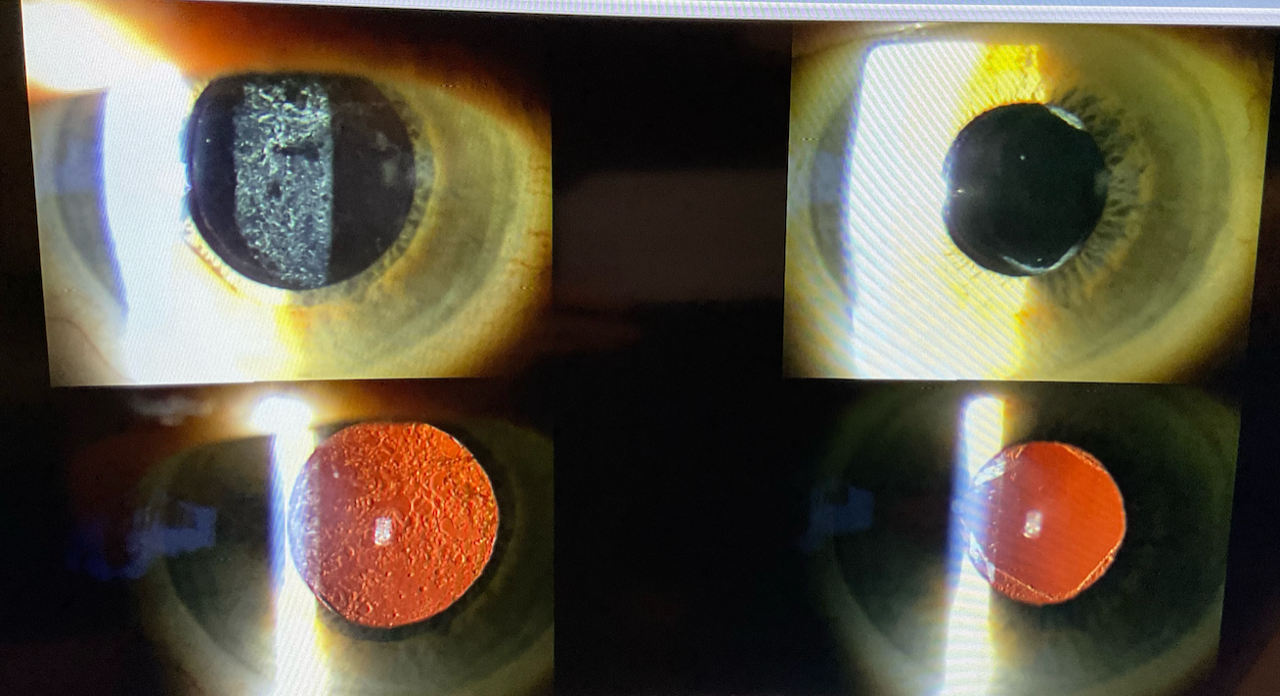
The photos on the left show the pre-op appearance of a patient with grade 3 posterior capsule opacification. The right two photos reveal the post-op appearance after a YAG capsulotomy was performed by an optometrist, showing perfect clearing of the posterior capsule. The patient’s vision was 20/20, and they were thrilled. Photo: Nate Lighthizer, OD. Click image to enlarge. |
“Optometrists have four to five years of rigorous classroom, laboratory and clinical training on these procedures—not ‘less than one year of training’ as was stated in the governor’s veto announcement,” says Nate Lighthizer, OD, associate dean at NSU Oklahoma College of Optometry and one of optometry’s chief advocates for scope expansion. Dr. Lighthizer routinely conducts training sessions on advanced procedures for optometrists across the country.
While disappointing, this development will not curtail scope expansion efforts in California and beyond. It does, however, underscore the importance of emphasizing training and education, which is fundamental to success for those performing the procedures, as well as the groups crafting legislation for other states. To see optometrists and advocates in more states have success in their endeavors to expand the scope of practice, it will be crucial to continually educate the community and lawmakers on the safety and importance of adding advanced procedures to optometry’s scope.
“It can take time and a lot of effort, but the patient is the reason for it,” says Dr. Day. “Even when a state’s optometric laws do change, it can still take some time for things to ‘ramp up.’ State boards must go through the process of rulemaking to ensure public safety.” Your job as the practitioner, Dr. Day notes, is to “purchase the necessary equipment and implement proper staff training and office protocols to deliver consistent and successful treatment.”
Credentialing Requirements
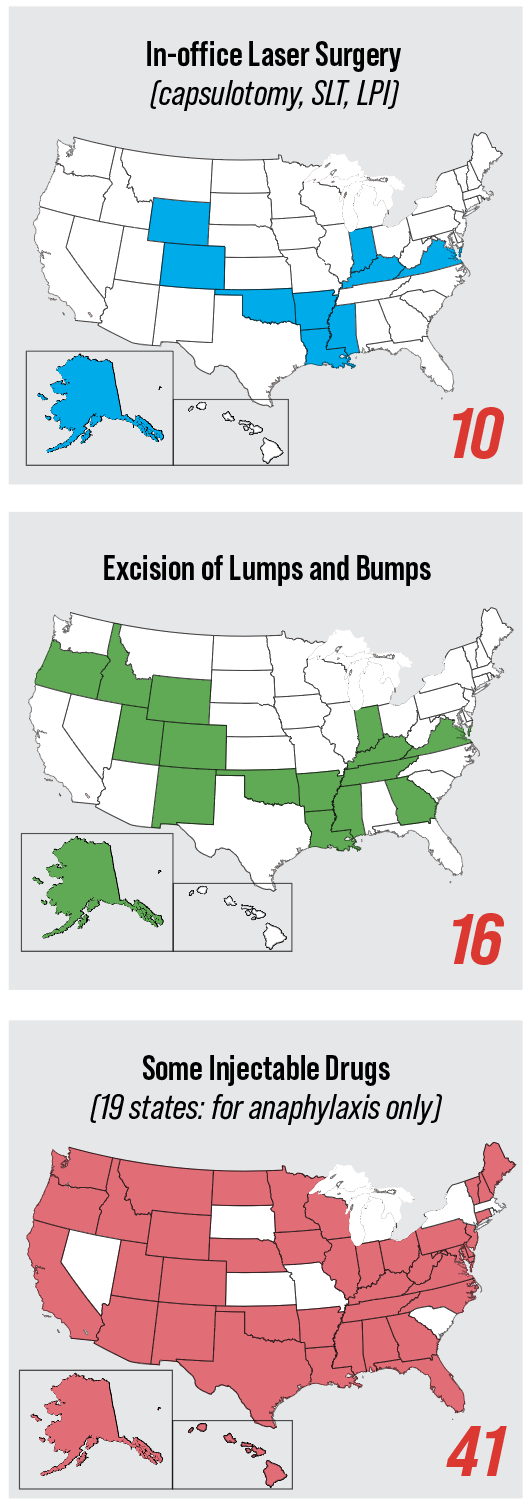 |
| The maps above display the states where laser surgery, lesion excision and injections are currently part of the optometric scope of practice. Colorado and Virginia are the two newest additions to the laser and lesion maps, having won those rights in 2022. Click image to enlarge. |
The first—and arguably most important—factor to consider when offering additional procedures at your clinic is whether additional certification or education is required. The credentialing process will differ by state, so it’s crucial that ODs connect with their state optometric associations to ensure they take the necessary steps. Below, we discuss specific requirements in three states with recent scope expansion legislation.
Wyoming. In April 2021, Wyoming passed legislation that expanded optometric scope of practice to include YAG laser capsulotomy, SLT, laser iridotomy and lesion removal. It also amended optometrists’ drug prescribing authority and granted board authority.
According to Kari Cline, executive director of the Wyoming Optometric Association (WOA), ODs in Wyoming interested in performing these procedures must complete one of the following education and examination requirements:
- graduate from an accredited college or university of optometry where the laser procedures and adnexa treatment were taught, as well as pass the National Board of Examiners in Optometry (NBEO) Laser and Surgical Procedures Examination; or
- complete a Wyoming State Board of Examiners in Optometry approved training course on laser and adnexa of eye procedures.
No additional proctoring is required for treatment of adnexa procedures; however, laser procedures require a proctored session within two years of completing the education requirement prior to performing laser surgical procedures. Proctoring may be performed by an optometrist or ophthalmologist licensed for these procedures.
“The WOA is committed to providing ongoing continuing education (CE) for ODs to stay updated on all the procedures,” notes Ms. Cline. “We have CE conferences twice a year in which we offer a variety of courses in lasers and minor surgical procedures.”
Some optometrists in Wyoming have already begun to offer the new procedures at their practice, according to Dr. Day. “Whether it’s the removal of a benign periocular skin lesion or SLT, many more patients can now receive treatment by their established eyecare provider with whom they have a trusted doctor-patient relationship,” he says. He also points out that the scope expansion has helped reduce travel and waiting times for patients in need of timely care. “We have had many instances where patients put off having a needed procedure because of travel time or worrisome travel conditions that often develop here in Wyoming. When a patient can have some of these things taken care of locally, it makes his or her life better.”
Mississippi. Under HB 1302, which went into effect in July 2021, ODs in Mississippi now have the authority to perform injections, remove non-cancerous lid lesions and perform laser capsulotomy. Per the legislation, optometrists must meet the following requirements, explains Sarah Link, executive director of the Mississippi Optometric Association (MOA):
- Provide proof of current Mississippi license to practice therapeutic optometry that is in good standing.
- Provide proof of satisfactorily completing a Primary Eyecare Procedures (PEP) course of instruction as approved by the Mississippi State Board of Optometry (MSBO). The course of instruction must be provided by an accredited optometry, osteopathy or medical school; be a minimum of 32 hours in length; and be sponsored by an organization approved by MSBO.
- Complete and pass a written test.
- Pass a clinical skills assessment approved by MSBO.
- Participate in an eight-hour preceptorship with an MSBO approved preceptor.
- Any other requirements as directed by MSBO.
“All procedures included under HB 1302 require the full credentialing process before an optometrist is authorized to perform said procedures,” says Ms. Link. “HB 1302 also authorizes all therapeutic licensed ODs (not just PEP-credentialed ODs) to prescribe drug schedules II to V (expanded from the previously authorized schedules IV to V). To prescribe the additional drug schedules, an optometrist must update their DEA registration card,” she notes.
 |
|
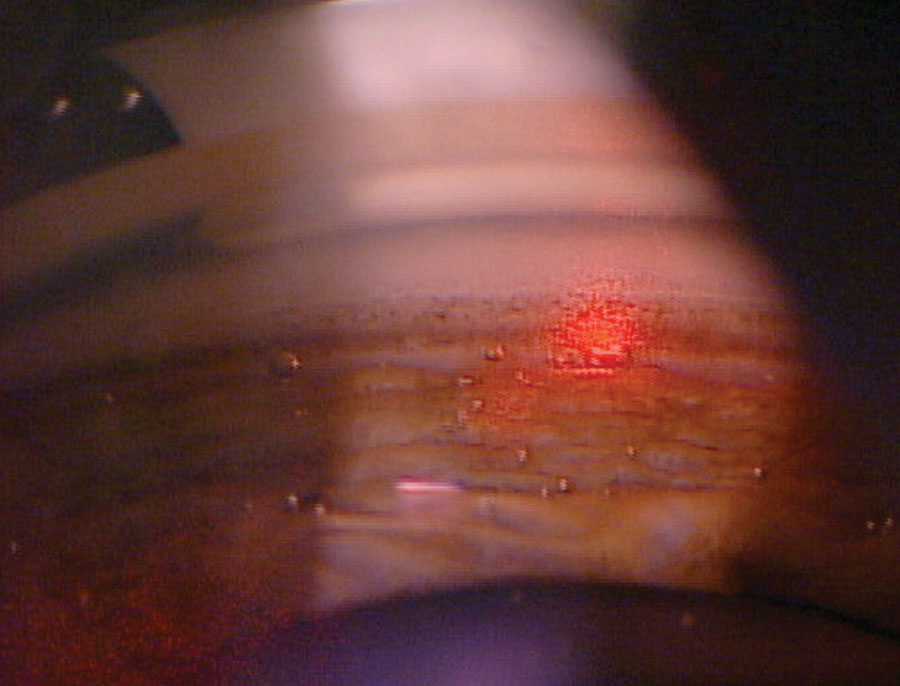
ODs in 10 states can perform various laser procedures, including SLT (pictured here), a quick and effective way to lower IOP in glaucoma patients. Photo: Nate Lighthizer, OD. Click image to enlarge. |
The credentialing process is the same for newer ODs whose education included the required training for these procedures, with one exception: the documentation for the training course. For those who graduate after 2021, the accredited school of optometry may turn in an affidavit to MSBO on behalf of the OD attesting to the equivalent completion of the 32-hour course as part of their training, according to Ms. Link. Optometrists who graduated in 2021 or before must complete the full 32-hour training process.
To maintain the PEP credential, an OD must complete six hours of CE focused on PEP procedures (as part of their overall licensing renewal requirements). Regardless of PEP credentialing, ODs in Mississippi are now required to complete a two-hour course on the prescribing and diversion of narcotics—in addition to existing licensing renewal requirements—every two years.
“The MOA has sponsored three PEP courses in 2021 and 2022, partnering with the Southern College of Optometry,” notes Ms. Link. “Moving forward, the MOA will periodically survey members to assess the necessity of future PEP courses.
“PEP training courses are also offered periodically throughout the United States by other state optometric associations, and MOA will keep members informed of said training courses,” she adds. “Every OD in Mississippi benefits from the new bill, whether or not they proceed with the PEP credentialing, which has the potential to benefit patients statewide.”
Kris May, OD, legislative chair of MOA, credits the MSBO and the MOA as driving forces behind the successful implementation of the state’s recent legislation. “They did a fantastic job making sure that the certification process was complete, rigorous and upholds the highest standards while preparing the practitioner and their office staff to take on the expanded scope of practice.”
Colorado. In June 2022, Colorado claimed the title of the most recent state to pass optometric scope expansion legislation. Under HB 22-1233, the state’s optometrists gained the authority to perform certain advanced procedures such as lesion removal, injections and CXL, as well as three laser procedures: YAG capsulotomy, laser peripheral iridotomy (LPI) and SLT.
Permanent education and training requirements were adopted by the state’s board of optometry in November. Per these rules, which take effect on January 14, 2023, ODs in Colorado will have to complete a board-approved 32-hour course, which includes at least six hours of hands-on clinical proctoring, according to Deanna Alexander, OD, legislative chair for the Colorado Optometric Association (COA). Doctors will have to maintain proof of completion and provide it to the board upon request.
“If more than two years lapse between laser procedures, an optometrist will have to repeat a clinical proctoring session with a currently certified optometrist or an ophthalmologist in any jurisdiction before they can do more procedures,” notes Dr. Alexander. “Additionally, ODs must report adverse outcomes to the state board of optometry.”
Optometrists who have graduated in 2019 or later and passed a standardized national exam specified by the state board are considered certified and can perform the new procedures as of January 14, 2023, says Heather Gitchell, OD, a member of the COA legislative team. “If the OD graduated in 2019 or later but did not pass the laser and surgical procedures portion of the NBEO exam, they must follow the same process as every other OD seeking certification.”
Since all the components of CXL were already a part of Colorado’s scope of practice—debridement of cornea, use of drops and use of light—no additional training is required to perform this procedure beyond manufacturer requirements for certain equipment.
 |
|
For Colorado ODs who recently gained the right to perform CXL, no additional training is necessary since the required skills were already part of the scope of practice. Photo: Glaukos. Click image to enlarge. |
There are a variety of educational opportunities available to Colorado ODs who want to expand the services they provide. To date, the COA has coordinated and planned two different courses taught by the NSU Oklahoma College of Optometry faculty in Colorado. The first was held this past summer and the second will be offered in February 2023 in Colorado Springs.
“Courses that meet the board’s educational and training requirements are also routinely offered at NSU Oklahoma College of Optometry and the Kentucky College of Optometry, and periodically at other locations around the country,” notes Dr. Alexander. “The COA will continue to offer courses locally until all Colorado ODs who wish to be certified are enrolled in the course.”
When discussing the scope expansion in Colorado, Dr. Gitchell emphasizes that the intent of the legislation and initial DORA report was to allow Colorado optometrists to practice in line with their education and training, not create areas where new skills had to be learned.
“The various advanced procedures courses are an extension of our current education and training rather than the introduction of new knowledge,” Dr. Gitchell says. “The techniques, safety protocols and management of complications for all these procedures are built into current optometric education and have been for decades.”
With a looming shortage of ophthalmologists and an aging patient population, there is a need for other providers to offer a broader scope of in-office care, and optometrists are in the perfect position to fill that gap, according to Dr. Alexander.
“Optometrists have a full-time presence in more counties in Colorado than ophthalmologists,” she says. “Approximately 70% of Colorado ODs are enrolled as Medicaid providers, which will improve access to care for those most in need.”
Top Considerations
How to Prep Your ClinicIncorporation of new procedures depends partly on the tools at your disposal. While the tools needed for individual practices will vary, Dr. Brog offers some suggestions to get started. He points out that this list is not exhaustive; there are many lens and tool options for ODs to consider investing in. Supplies list for benign lesion removal:
Supplies list for YAG capsulotomy/SLT/LPI:
|
When you’re ready to take the leap and add minor procedures such as lesion removal or laser surgery to your practice, you’ll need to check several boxes to ensure you, your staff and your patients are prepared. Below, we discuss some of the key considerations, including stocking the equipment, educating staff and addressing administrative concerns.
Equipping your clinical practice. The exact tools and equipment you decide to invest in will depend on the specific needs of your practice, with factors such as budget and patient demand to consider. For minor surgical procedures, such as lesion removal, the initial investment doesn’t have to break the bank (see “How to Prep Your Clinic” for a list of recommended tools).
“Getting started is a very practice-specific process,” notes Dr. May. “For instance, equipment acquisition can be a significant investment. Your patient base will guide you; an office with a large geriatric population in a remote area may have very high demand for YAG capsulotomy, whereas a heavy pediatrics practice may not have any demand at all,” he points out. “The same is true for space allocation within the office. Some clinics are adding dedicated rooms for lid procedures and sterilization equipment while others are using more portable equipment and disposables.”
One of the first decisions for ODs adding laser surgery to their practice is whether to invest in a laser for their clinic or find another way to gain access to this vital piece of equipment. “If I were a doctor in Colorado, Virginia or one of the other states who recently gained the authority to perform laser procedures, I would purchase a combination YAG/SLT laser,” says Dr. Lighthizer. “The more optometrists who have lasers in their practice and are performing laser surgery, the more that laser procedures become embedded into the DNA of optometry.”
“One common misconception within optometry is that lasers are beyond the profession’s reach to purchase,” says Chris Wroten, OD, a member of the Louisiana State Board of Optometry Examiners who practices full-scope optometry in that state. “Even brand new, a combination YAG/SLT laser from any of the major manufacturers is less expensive than an OCT. Further, many manufacturers offer their own refurbished lasers at a discount from time to time, not to mention the deep discounts available on secondhand lasers offered by established and reputable after-market sellers,” he says.
For ODs who aren’t yet ready or prefer not to purchase a laser, there are several alternative options to consider, such as working with a local ambulatory surgery center (ASC), suggests Aaron McNulty, OD, who practices at Louisville Eye Center in Kentucky. Optometrists can go to the ASC to perform laser procedures, and, in those cases, the OD would bill for the surgical fee, while the ASC bills a facility fee, he explains. ODs could also partner with a nearby optometric colleague and purchase a laser together, allowing them to share the financial burden while still ensuring they have access to needed equipment. Another option would be working with a company and renting a laser as needed.
Staff education and buy-in. No matter the type of procedure(s) being integrated into clinical practice, a key factor to providing excellent patient care is staff education, says Dr. May. “In the same way that each of the doctors are certified in PEP, the staff needs to be trained in supporting those procedures. This ranges from understanding procedures so that patients feel at ease to updating Occupational Safety and Health Administration protocols and maintaining safety,” he explains.
Dr. McNulty recognizes that when optometrists begin offering these procedures—whether it is laser or minor surgery—they are ready and willing to do a lot of the legwork themselves, but he notes that in the long term, this isn’t realistic. “Integrating these services into the daily and weekly flow of a busy optometry office will require significant delegation,” he says. “A lot of the pre- and post-op work can be delegated for maximum efficiency; however, doing so safely will depend on having highly trained staff who are equipped to take on those responsibilities.”
Luke Brog, OD, an optometrist who practices in Wyoming and a member of the WOA Legislative Committee, actively involved his entire staff in the implementation process. “We still share a great bond when we have patients who come in for these procedures because we worked on it together,” he says. “One of my staff members suggested we color-code the different procedures on the schedule. We gave each a different color, so a quick look at the schedule tells us how many procedures and which procedures we will be doing that day or week.”
Dr. Brog put together a list of steps for himself and staff to follow before, during and after each procedure. One of his staff members then took the initiative to format it so it was easier to follow, and these lists have since become quick reference guides to help his office get all of the equipment ready for each procedure performed. “These checklists have been really helpful for the staff members and practice flow,” he says. “In cases when there’s a different staff member helping than usual, these lists have been invaluable.”
By including his staff from the start of the implementation process, Dr. Brog not only ensured his team was prepared and ready to assist with these procedures, but he also fostered an environment of team accountability and support. “We all came together and worked through the details of how we would best implement these new procedures into the office,” Dr. Brog notes. “We have hired new staff members since we started performing these procedures. The staff that has been with us from the beginning love to train the new members of our team. They get excited, and that creates excitement for new hires.”
Administrative and insurance concerns. There are a variety of administrative-related logistics that an OD must be aware of when implementing services into practice. For instance, having consent forms on hand for each new procedure is key, notes Dr. Lighthizer. If ODs are looking for examples, he recommends visiting the Ophthalmic Mutual Insurance Company website (www.omic.com).
Another important consideration to address before performing any of these procedures is malpractice insurance. “It is imperative that you check with your malpractice insurance carrier to make sure that these procedures are covered under your current policy,” says Dr. Lighthizer. “You certainly don’t want to be performing laser procedures and then find out after the fact that they’re not covered.”
 |
|
Lesion excision is increasingly being recognized as part of optometry’s scope of practice, currently permitted by 16 US states. Photo: Jackie Burress, OD, and Rodney Bendure, OD. Click image to enlarge. |
Patient outreach. As you navigate the clinical and administrative logistics of adding these services into practice, you also must dedicate time to patient outreach and education. Make sure both established and new patients, as well as community members, are aware that they can now come to your office for these procedures.
“When you are attending local fundraisers or events, talk about your practice and what you offer,” recommends Dr. Lighthizer. “In your office, place signage and brochures that highlight the new procedures and how they can benefit the various needs of your patients.”
Reaching out to fellow ODs in your area can also be an effective approach. “Not every optometrist is going to have an interest in performing every procedure,” says Dr. Lighthizer. “So, communicate to your colleagues that you would be happy to perform these procedures and then send their patient back to them. We can, and should, support one another whenever possible.”
Optometric scope expansion provides value to ODs, patients and the community at large. “As scope expansion continues to take place, more and more optometrists will provide these services, and people will be able to gain easier access to comprehensive eye care,” notes Dr. Brog. “As for myself, it is really fulfilling to someone that is seeing 20/200 to 20/400, and in a few minutes with the YAG laser, help them to see 20/20 again.” He continues, “Scope expansion has been a wonderful addition to my practice. It’s a great feeling to be able to better help patients with their eyecare needs.”
Looking Ahead
As scope expansion continues across the country, optometrists must lean on and learn from one another together to ensure everyone is prepared for the mantle of responsibility that comes with additional practice authority. This includes ongoing legislative, regulatory, educational and community outreach efforts. In states that have already gained expanded practice authority, proper implementation of new legislation can set an example and pave the way to success in other states.
