 |
A 69-year-old white male presented for a routine eye exam without any ocular complaints. His ocular history was remarkable for a superficial corneal foreign body with removal and no complications over five years ago. His systemic history was remarkable for hypertension and benign prostatic hyperplasia, for which he was properly medicated. He reported no allergies.
Clinical Findings
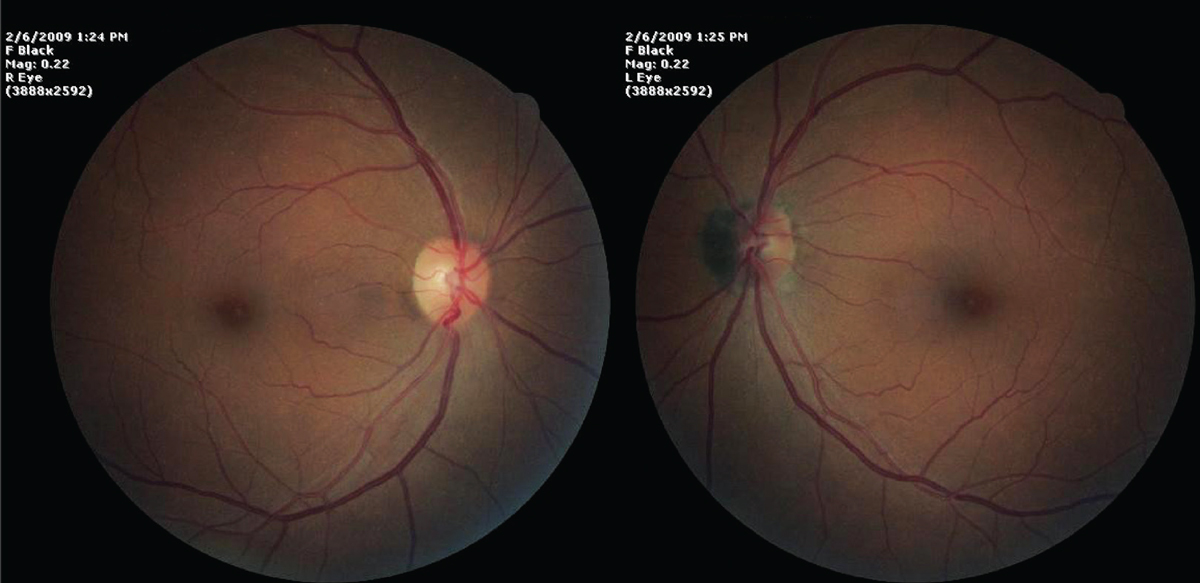
The patient’s best-corrected entering visual acuity measured 20/20 OD and 20/20 OS at distance and near. His external examination was normal, confrontation visual fields were full and there was no afferent pupillary defect. The anterior segment biomicroscopic exam demonstrated normal structures with mild cataracts and Goldmann applanation pressures that measured 13mm Hg OU. The pertinent fundus findings from the dilated posterior segment examination are demonstrated in the photographs.
For More Information
Additional tests for this case might include a spectral-domain or swept-source OCT of the optic nerve OS to determine the depth of tissue and vasculature involvement, Amsler grid testing OU to rule out metamorphopsia OS, B-scan ultrasonography OS to better understand the extent of the lesion and visual field testing to rule out any functional deficits.
A frequency-doubling perimetry test was completed and found to be normal, OU. Referral to a retina specialist is prudent even in the event the diagnosis is known.
 |
|
Fundus exam findings in our patient. What do these images suggest to you? Click image to enlarge. |
Magnocellular Nevus
The diagnosis in this issue is large melanocytoma, also known as magnocellular nevus, of the optic disc. A melanocytoma of the optic disc is defined as a unilateral benign ocular tumor composed of melanocytes involving the optic disc and the surrounding retina and choroid.1-21 The average age at diagnosis is 50 and the condition is seen slightly more commonly in females.1,3,9 The lesion itself appears dark brown or black overlying the optic nerve and is generally smaller than the disc (< 2mm in diameter and 1mm in thickness).2 It may grow slowly over time and has a 1% to 2% chance of malignant transformation into melanoma.1,3
Melanocytoma lesions contain pigmented round nevus cells.1 Although this condition has been noted as congenital, cases are rarely seen in children, suggesting an acquired pathology such as pigmentation of an amelanotic congenital lesion.1
Potential growth has the ability to affect the vasculature and nerve fibers that surround the optic nerve, resulting in a variety of functional deficits and visual complications.6
Clinical Manifestations
The condition’s impact on vision varies. Lee et al. found that 93% of patients with this condition had consistent vision of 20/40 or better.3 However, depending on the extent of optic nerve involvement, vision may deteriorate to no light perception in the affected eye.3,9,11,17,19 If vision begins to slowly deteriorate in the affected eye, suspicion should be raised for malignant changes.
The extent to which optic nerve melanocytomas affect the visual field also differs. Depending on the location and extent of the lesion, a melanocytoma may compress the axons in the optic nerve head, causing visual field loss with as high as 90% of all cases of melanocytoma being associated with visual field disturbances.1,9,10,13,14,16,18 Interestingly, blood vessel network location within this benign tumor seems to correspond directly to the location of a visual field defect.4 Therefore, it is crucial to obtain baseline visual field results and monitor them regularly, as sudden changes in visual fields can also signify vascular and malignant changes.1,9,10,13,14,16,18
Next Month in the MagIn July, we present our annual glaucoma report. Articles will include:
Also in this issue:
|
Another clue to malignant transformation is afferent pupillary defect (APD).3 An APD in the presence of a melanocytoma is likely the result of optic nerve fiber and axon compression.3
Prior to 1962, melanocytomas were commonly mistaken as malignant melanomas, resulting in enucleation of the affected eye.1 Today, it is easier to distinguish a melanocytoma from malignant melanoma. Malignant melanomas are usually more than 1.5mm in thickness and often contain subretinal fluid.3 They appear with overlying orange pigment.3
A multitude of OCT studies have shed some light on malanocytoma malignant transformation.5,7,13,15,17 It has been demonstrated that a higher degree of tumor neovascularization, complicated vascular patterns and blood vessel leakage (seen with fluorescein angiography) is associated with a higher chance of progression to malignant melanoma.7,13,15,17
There is no treatment for optic nerve melanocytoma; rather, patients should continue to return at eight- to 12-month intervals for a dilated fundus examination, OCT scan, photodocumentation, ultrasound (to monitor internal reflectivity) and automated perimetry to monitor for any progression of functional loss, growth or pathologic progression.1,8,12,20
This patient was referred to the retina service, where the diagnosis was confirmed. He continues to return yearly for these studies and has remained stable for a number of years.
Dr. Gurwood thanks Oskar Shura, HBsc, Virginia Donati, OD, FCOVD, and Michelle McKenzie, OD, FCOVD, for contributing this case.
Dr. Gurwood is a professor of clinical sciences at The Eye Institute of the Pennsylvania College of Optometry at Salus University. He is a co-chief of Primary Care Suite 3. He is attending medical staff in the department of ophthalmology at Albert Einstein Medical Center, Philadelphia. He has no financial interests to disclose.
1. Shields JA, Demirci H, Mashayekhi A, et al. Melanocytoma of the optic disk: a review. Surv Ophthalmol. 2006;51(2):93-104. |
